

ņä£ļĪĀ
Ļ░æņāüņäĀ ņŚ¼ĒżņĢöņØĆ ņĀäņ▓┤ Ļ░æņāüņäĀ ņĢö ņżæ ņĢĮ 10-15%ļź╝ ņ░©ņ¦ĆĒĢśļ®░, ļæÉļ▓łņ¦ĖļĪ£ ĒØöĒĢ£ ņ£ĀĒśĢņØ┤ļŗż. Ļ░æņāüņäĀ ņŚ¼ĒżņĢöņØĆ ņŚ¼ņ×ÉņŚÉņä£ ļ¦ÄņØ┤ ļ░£ņāØĒĢśļ®░, ļ░£ļ│æ ĒÅēĻĘĀ ņŚ░ļĀ╣ņØ┤ 40-50ļīĆ ņØ┤ņāüņØ┤ļŗż.1,2) ņØ┤ ņĢöņóģņØĆ ņ▓£ņ▓£Ē׳ ņ×ÉļØ╝ļŖö ņóģņ¢æņ£╝ļĪ£ņä£ ņøÉĻ▓®ņĀäņØ┤ļź╝ ļÅÖļ░śĒĢśņ¦Ć ņĢŖņØä ļĢī ņ¢æĒśĖĒĢ£ ņśłĒøäļź╝ ļ│┤ņØ┤ņ¦Ćļ¦ī,3) ņøÉĻ▓®ņĀäņØ┤ļŖö ņŻ╝ļĪ£ ĒÅÉ, Ļ│©, ļćī ļō▒Ļ│╝ ĒĢ©Ļ╗ś ĻĖ░ĒāĆ ņŚ░ņĪ░ņ¦üņŚÉļÅä ņØ╝ņ¢┤ļéĀ ņłś ņ׳ļŗż.4) Ļ│© ņĀäņØ┤ļŖö ņ▓ÖņČö, Ļ│©ļ░ś, ļŖæĻ│© ļ╣łļÅäļĪ£ ļ│┤Ļ│ĀļÉśļ®░, ļæÉĻ░£Ļ│©ņŚÉ ņĀäņØ┤ļÉśļŖö Ļ▓ĮņÜ░ļŖö ļ¦żņÜ░ ļō£ļ¼╝ļŗż.5-7)
ņĀĆņ×ÉļōżņØĆ Ļ░æņāüņäĀ ņÜ░ņŚĮņØś Ļ▒░ļīĆ ņóģļ¼╝Ļ│╝ ļ│äļÅäņØś ņóģņ¢æņ£╝ļĪ£ ņČöņĀĢļÉśļŖö ņóīņĖĪ ņĢłņÖĆņØś ņóģļ¼╝ļĪ£ ļé┤ņøÉĒĢ£ ĒÖśņ×ÉņŚÉņä£, Ļ░æņāüņäĀ ņŚ¼ĒżņĢö ļ░Å ļŗ©ņØ╝ ņĀäņØ┤ņä▒ ļ│æļ│ĆņØä ĒÖĢņØĖĒĢśņśĆĻ│Ā ņČöĒøäņŚÉ ļŗżļ░£ņä▒ Ļ│© ņĀäņØ┤ļź╝ ĒÖĢņØĖĒĢ£ ņ”ØļĪĆļź╝ Ļ▓ĮĒŚśĒĢśņśĆĻĖ░ņŚÉ ļ¼ĖĒŚī Ļ│Āņ░░Ļ│╝ ĒĢ©Ļ╗ś ļ│┤Ļ│ĀĒĢśļŖö ļ░öņØ┤ļŗż.
ņ”ØļĪĆ
74ņäĖ ņŚ¼ņ×É ĒÖśņ×ÉĻ░Ć ļé┤ņøÉ 40ļģä ņĀäļČĆĒä░ ņ¦ĆņåŹļÉ£ ņÜ░ņĖĪ ņĀäĻ▓ĮļČĆ ņóģļ¼╝ņØ┤ 1ļģä ņĀäļČĆĒä░ ĻĖēĻ▓®Ē׳ Ēü¼ĻĖ░Ļ░Ć ņ”ØĻ░ĆļÉśņ¢┤ ļ│ĖņøÉ ņØ┤ļ╣äņØĖĒøäĻ│╝ ņÖĖļלļĪ£ ļé┤ņøÉĒĢśņśĆļŗż. ĒÖśņ×ÉļŖö Ļ│ĀĒśłņĢĢ Ļ│╝Ļ▒░ļĀźņØ┤ ņ׳ņŚłĻ│Ā, ņŗĀņ▓┤Ļ▓Ćņ¦äņāü Ļ░æņāüņäĀ ņÜ░ņŚĮņØś ņĢĮ 7cm Ēü¼ĻĖ░ņØś ļ¼┤ĒåĄņä▒ ņóģļ¼╝ņØ┤ ņ┤ēņ¦äļÉśņŚłļŗż. Ļ▓ĮļČĆ ņĀäņé░ĒÖö ļŗ©ņĖĄ ņ┤¼ņśü Ļ▓Ćņé¼ņŚÉņä£ Ļ░æņāüņäĀ ņÜ░ņŚĮņØś ņןĻ▓Į 7.6cm Ēü¼ĻĖ░ņØś ļé┤ļČĆ Ļ┤┤ņé¼, ņŻ╝ļ│Ć ņäØĒÜīĒÖö, Ļ░æņāüņäĀņÖĖņ╣©ļ▓öņØä ļ│┤ņØ┤ļŖö ņóģļ¼╝ ņåīĻ▓¼Ļ│╝, ņóīņĖĪ ņĢłņÖĆ ņāüļ▓ĮņØś ļČłĻĘ£ņ╣ÖņĀüņØĖ ļ¬©ņ¢æņØś ļŗ©ņØ╝ņä▒ Ļ│©ļ│æļ│ĆņØ┤ ņÜ░ņŚ░Ē׳ ĒÖĢņØĖļÉśņŚłĻ│Ā ĻĖ░ĒāĆ Ļ▓ĮļČĆņØś ņĢģņä▒ ļ”╝ĒöäņĀł ņĀäņØ┤ ņåīĻ▓¼ņØĆ ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśļŗż. ļŗ©ņØ╝ņä▒ ņĢłņÖĆĻ│© ļ│æļ│ĆņØĆ ņśüņāü ĒīÉļÅģ ņåīĻ▓¼ņāü Ļ│© ņĀäņØ┤ļ│┤ļŗżļŖö ņĢģņä▒ ļ”╝Ēöäņóģ ļō▒ ļ│äĻ░£ņØś ņóģņ¢æņ£╝ļĪ£ ņØśņŗ¼ļÉśņŚłļŗż(Fig. 1). Ļ░æņāüņäĀ ņ┤łņØīĒīīĻ▓Ćņé¼ņŚÉņä£ Ļ░æņāüņäĀ ņÜ░ņŚĮ ņĀäņ▓┤ņŚÉ Ļ▒Ėņ│É ļé┤ļČĆ ļéŁņóģ, ļ»ĖņäĖ, Ļ▒░ļīĆ ņäØĒÜīĒÖö ĻĘĖļ”¼Ļ│Ā Ēśłļźśņ”ØĻ░Ćļź╝ ļÅÖļ░śĒĢ£ Ļ▓░ņĀłņØ┤ Ļ┤Ćņ░░ļÉśņŚłĻ│Ā, ņäĖņ╣©ĒØĪņ×ģņäĖĒżĻ▓Ćņé¼ņŚÉņä£ Ļ░æņāüņäĀ ņÜ░ņŚĮ ņóģļ¼╝ņØĆ Ļ░æņāüņäĀ ņŚ¼Ēż ņóģņ¢æņ£╝ļĪ£ ĒÖĢņØĖļÉśņŚłļŗż. ļŗ©ņØ╝ņä▒ ņĢłņÖĆĻ│© ļ│æļ│ĆņØĆ ņĢģņä▒ ļ”╝Ēöäņóģ ļō▒ ļ│äĻ░£ņØś ņ¦łĒÖśņ£╝ļĪ£ Ļ│ĀļĀżĒĢśņŚ¼ Ļ░æņāüņäĀ ņÜ░ņŚĮņĀłņĀ£ņłĀņØä ņÜ░ņäĀ ņŗ£Ē¢ēĒĢśņśĆļŗż. ņĀüņČ£ļÉ£ ņĪ░ņ¦üņØś ļ│æļ”¼ ņ£ĪņĢł ņåīĻ▓¼ņŚÉņä£ ĒÜīņāēļ╣øņØś ļŗ©ļŗ©ĒĢ£ ņĀłļŗ©ļ®┤ņØä Ļ░Ćņ¦ä Ļ▓ĮĻ│äĻ░Ć ļ¬ģĒÖĢ(well- circumscribed)ĒĢ£ ĒāĆņøÉņØś ņóģļ¼╝ņØ┤ ņĄ£ņן 6cmņØś Ļ░æņāüņäĀ ņÜ░ņŚĮņØä Ļ▒░ņØś ņ░©ņ¦ĆĒĢśļŖö ņ¢æņāüņØ┤ņŚłļŗż(Fig. 2, 3A). Ēśäļ»ĖĻ▓Į ņåīĻ▓¼ņŚÉņä£ ņóģļ¼╝ņØĆ ņä¼ņ£Āļ▓ĮņØś Ēö╝ļ¦ēņ£╝ļĪ£ ļæśļ¤¼ņŗĖņśĆņ£╝ļ®░, Ēö╝ļ¦ē ņ╣©ņŖĄ ļ░Å ĒśłĻ┤Ć ņ╣©ņŖĄņØ┤ ļ│┤ņŚ¼ Ēö╝ļ¦ēņä▒ ĒśłĻ┤Ćņ╣©ņŖĄ ņŚ¼ĒżņĢö(encapsulated angioinvasive follicular carcinoma)ņ£╝ļĪ£ ņ¦äļŗ©ļÉśņŚłļŗż(Fig. 3B, 3C).
Fig.┬Ā1
Preoperative axial CT findings. About 6.6 x 5.5 x 7.6 cm sized thyroid mass in right lobe with internal necrosis, peripheral calcification and extrathyroidal extension causing tracheal deviation to left(A: white arrow, CT) and Irregular shaped bone lesion in left orbital roof(B: white arrowhead, CT)
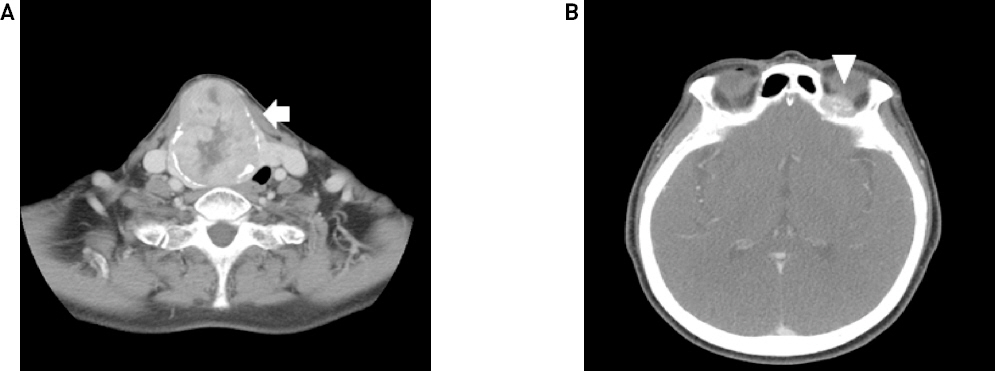
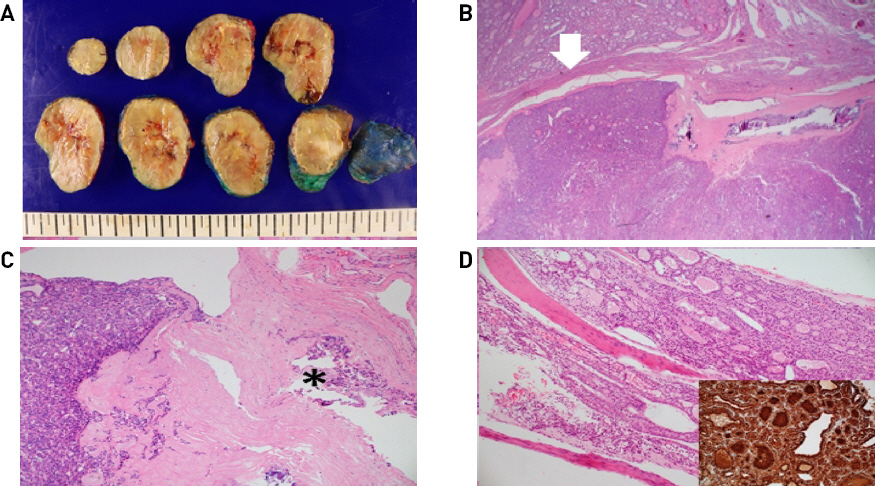
Fig.┬Ā2
Gross photograph of surgical specimen showing 6cm sized mass occupying almost the entire right thyroid.

Fig.┬Ā3
(A) Serial sections of right lobe of thyroid gland showing a well-circumscribed, ovoid mass with grayish solid cut surface, central cystic change and peripheral calcification, occupying almost the entire thyroid lobe. (B) The mass is encapsulated by a fibrous wall with capsular invasion(white arrow) and focal calcification(H&E, x12.5). (C) The mass consists of predominant microfollicles (left side) and shows frequent vascular invasion(asterix) within the fibrous capsule(H&E, x100). (D) The mass from the orbital bone reveals infiltrated thyroid follicles within the bone marrow space, which are stained by thyroglobulin. (H&E, x 100, inset: thyroglobulin).
ņĪ░ņ¦üĻ▓Ćņé¼ Ļ▓░Ļ│╝ ĒÖĢņØĖ Ēøä ņ×öņĪ┤ Ļ░æņāüņäĀ ņóīņŚĮņĀłņĀ£ņłĀņØä Ļ│äĒÜŹĒĢśļ®░, ņĢöņØś ļ│æĻĖ░ ņäżņĀĢņØä ņ£äĒĢ£ ņśüņāüĻ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢśņśĆļŗż. ņłśņłĀ ņĀä Ļ▓ĮļČĆ ņĀäņé░ĒÖö ļŗ©ņĖĄ ņ┤¼ņśü Ļ▓Ćņé¼ļĪ£ ĒÖĢņØĖļÉśņŚłļŹś ļŗ©ņØ╝ņä▒ ņĢłņÖĆĻ│© ļ│æļ│ĆņŚÉ ļīĆĒĢśņŚ¼ ņĢłņÖĆ ņ×ÉĻĖ░Ļ│Ąļ¬ģņśüņāüņ┤¼ņśü ņŗ£Ē¢ēĒĢśņśĆĻ│Ā, ņóīņĖĪ ņĢłņÖĆ ņāüļ▓ĮņØś ņĢĮ 2.2cmņØś ņóģļ¼╝ņØ┤ ĒÖĢņØĖļÉśņŚłļŖöļŹ░ ņØ┤ļŖö Ļ│© ņĀäņØ┤ ļ│┤ļŗżļŖö ļ”╝Ēöäņóģ ņåīĻ▓¼ņØ┤ ļŹö ņØśņŗ¼ļÉśņŚłļŗż(Fig. 4). ņĀäņŗĀ ņ¢æņĀäņ×É ļ░®ņČ£ ļŗ©ņĖĄ ņ┤¼ņśü Ļ▓Ćņé¼ņāüņŚÉņä£ ņĢģņä▒ Ļ▓ĮļČĆ ļ”╝ĒöäņĀł ņĀäņØ┤ļź╝ ņØśņŗ¼ĒĢĀ ļ¦īĒĢ£ ņåīĻ▓¼ņØĆ ņŚåņŚłņ£╝ļéś ņóīņĖĪ ņĢłņÖĆ ņāüļ▓ĮņØś ņäŁņĘ© ņ”ØĻ░ĆņÖĆ ņóīņĖĪ ĒĢśņĢģĻ│©, ņÜ░ņĖĪ ņāüņÖäĻ│©, ņ¢æņĖĪ Ļ▓¼Ļ░æĻ│©, ĒØēņČö, ņÜöņČö, ņÜ░ņĖĪ 8ļ▓ł ļŖæĻ│©, ĒØēĻ│©, ņ▓£Ļ│©ņØś ļŗżļ░£ņä▒ Ļ│© ņäŁņĘ© ņ”ØĻ░Ć ņåīĻ▓¼ņØ┤ ļ│┤ņśĆļŗż(Fig. 5). ĻĘĖļ¤¼ļéś ņØ┤ņ¢┤ ņŗ£Ē¢ēĒĢ£ Ļ│©ņŖżņ║öņŚÉņä£ ņÜ░ņĖĪ ņāüņÖäĻ│©ņØś Ļ▓ĮļÅäņØś ņäŁņĘ© ņ”ØĻ░Ć ņåīĻ▓¼ ņØ┤ņÖĖņŚö ņØ┤ņāü ņåīĻ▓¼ņØĆ ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśļŗż(Fig. 6). ņØ┤ņŚÉ Ļ│© ņĀäņØ┤ Ēś╣ņØĆ ņĢģņä▒ ļ”╝ĒöäņóģņØś ļŗżļ░£ņä▒ ņ╣©ļ▓öņØś Ļ░Éļ│äņØä ņ£äĒĢśņŚ¼ ņĪ░ņ¦üĒĢÖņĀüņØĖ ĒÖĢņØĖņØ┤ ĒĢäņÜöĒĢśļŗżĻ│Ā ĒīÉļŗ©ĒĢśņŚ¼, ņ▓½ ņłśņłĀ ņŗ£Ē¢ē ĒĢ£ ļŗ¼ Ēøä ļŗ©ņØ╝ņä▒ ņóīņĖĪ ņĢłņÖĆĻ│© ļ│æļ│ĆņØĆ ļ│ĖņøÉ ņŗĀĻ▓ĮņÖĖĻ│╝ņÖĆ ņāüņØśĒĢśņŚ¼ ņĀ£Ļ▒░ĒĢ©Ļ│╝ ļÅÖņŗ£ņŚÉ ņ×öņĪ┤ Ļ░æņāüņäĀ ņóīņŚĮņĀłņĀ£ņłĀ ļ░Å ņżæņŗ¼ Ļ▓ĮļČĆ ļ”╝ĒöäņĀł ņĀłņĀ£ņłĀņØä ņŗ£Ē¢ēĒĢśņśĆļŗż. ņĪ░ņ¦ü Ēśäļ»ĖĻ▓Į ņåīĻ▓¼ņŚÉņä£ ņóīņĖĪ ņĢłņÖĆĻ│© ļ│æļ│ĆņØĆ Ēö╝ņ¦łĻ│© ļé┤ļĪ£ ņ╣©ņ£żļÉ£ Ļ░æņāüņäĀ ņŚ¼ĒżĻ░Ć ļ│┤ņØ┤ļ®░, Ēŗ░ļĪ£ĻĖĆļĪ£ļČłļ”░ ļ®┤ņŚŁņŚ╝ņāēņØ┤ ņ¦äļŗ©ņŚÉ ļÅäņøĆņØ┤ ļÉśņ¢┤, ļ”╝ĒöäņóģņØ┤ ņĢäļŗī ņĀäņØ┤ņä▒ Ļ░æņāüņäĀ ņŚ¼ĒżņĢöņ£╝ļĪ£ ņ¦äļŗ©ļÉśņŚłļŗż(Fig. 3D).
Fig.┬Ā4
Preoperative coronal T1-weighted MR findings. About 2.2cm left orbital roof mass with irregular shape. (white arrow, T1W enhanced MRI)
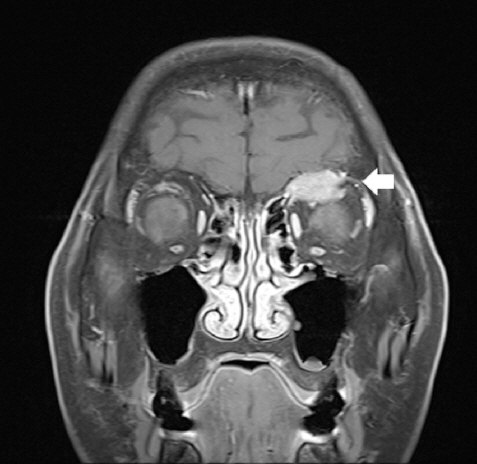
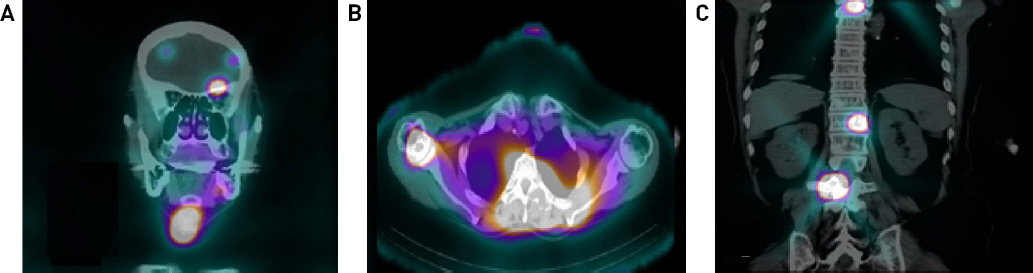
Fig.┬Ā5
Preoperative axial and coronal PET-CT findings. Multiple hypermetabolic mass were noted at (A) left orbital area(arrow), (B) humeral head, (C) T1, T3, T4, T12 and L3 spine.

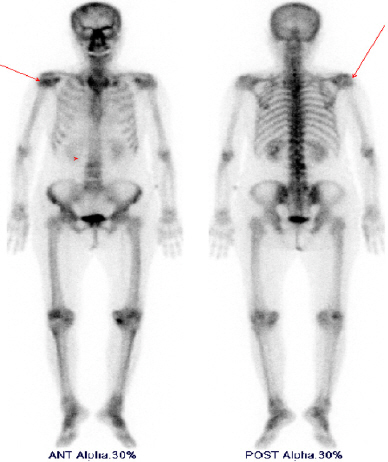
Fig.┬Ā6
Preoperative Bone scan shows mildly increased radiouptake in right humeral head (red arrow).
ņĄ£ņóģņĀüņ£╝ļĪ£ Ļ░æņāüņäĀ ņŚ¼ĒżņĢöņØś ļŗżļ░£ņä▒ Ļ│© ņĀäņØ┤(pT3N0M1) ņ¦äļŗ© ĒĢśņŚÉ ņłśņłĀ 3Ļ░£ņøö Ēøä 200mCiņØś ĻĘ╝ņ╣śņĀü ļ░®ņé¼ņä▒ ņÜöņśżļō£ ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢśņśĆĻ│Ā, ņ╣śļŻī ņóģļŻī Ēøä Ļ▓ĮļČĆ SPECT/CTņāüņŚÉ ņĢäņ¦ü ņóīņĖĪ ņĢłņÖĆĻ│©, ņÜ░ņĖĪ ĒøäļæÉĻ│©, ņÜ░ņĖĪ ņāüņÖäĻ│©, ĒØēņČö, ĒØēĻ│©, ņóīņĖĪ 6ļ▓ł ļŖæĻ│©, ņÜ░ņĖĪ 8ļ▓ł ļŖæĻ│©, ņ▓£Ļ│©, ņÜ░ņĖĪ ļīĆĒć┤Ļ│©, ņÜ░ņĖĪ ņĀäļæÉņŚĮņØś ļŗżļ░£ņä▒ ņĀäņŗĀ ņĀäņØ┤ ņåīĻ▓¼ņØä ĒÖĢņØĖĒĢśņśĆļŗż(Fig. 7). ņØ┤ņ¢┤ ļ│ĖņøÉņŚÉņä£ ņČöĻ░Ć ņ╣śļŻī Ļ│äĒÜŹ ņżæ ĒÖśņ×É ņŚ░Ļ│Āņ¦Ć Ļ┤ĆĻ│äļĪ£ ĒāĆļ│æņøÉņ£╝ļĪ£ ņĀäņøÉņØä ĒĢśņśĆĻ│Ā, 1ņ░© ļ░®ņé¼ņä▒ ņÜöņśżļō£ ņ╣śļŻī ņŗ£Ē¢ē 6Ļ░£ņøö Ēøä 2ņ░© ļ░®ņé¼ņä▒ ņÜöņśżļō£ ņ╣śļŻīļ░øĻ│Ā, Ēśäņ×¼ ĒÖśņ×É ņĀäņŗĀ ņ¢æĒśĖĒĢ£ ņāüĒā£ļĪ£ ņāØņĪ┤ ņżæņØ┤ļŗż.
Fig.┬Ā7
Postoperative I-131coronal and axial SPECT/CT findings. (A) Increased radioactive iodine uptake in left orbital bone with calcified soft tissue mass formation, right frontal lobe of brain and right thyroid operation bed. (B) Increased radioactive iodine uptake in right humerus. (C) Increased radioactive iodine uptake in T3, T12, L3 spine.
Ļ│Āņ░░
Ļ░æņāüņäĀ ņŚ¼ĒżņĢöņØĆ Ļ░æņāüņäĀ ņ£ĀļæÉņĢöĻ│╝ ļŗżļź┤Ļ▓ī ļ╣äĻĄÉņĀü ļåÆņØĆ ļ│æĻĖ░ņŚÉņä£ ņ▓śņØī ļ░£Ļ▓¼ļÉśĻ│Ā, ņĀäņŗĀ ņĀäņØ┤Ļ░Ć ĒØöĒĢśĻ▓ī ļÅÖļ░śļÉśļŖö Ļ▓ĮĒ¢źņØ┤ ņ׳ļŗż. Ļ░æņāüņäĀ ņŚ¼ĒżņĢöņØś ņøÉĻ▓® ņĀäņØ┤ļŖö Ļ│© ņĀäņØ┤Ļ░Ć ĒÅÉ ņĀäņØ┤ ļŗżņØīņ£╝ļĪ£ ļæÉ ļ▓łņ¦ĖļĪ£ ĒØöĒĢśĻ▓ī ļ░£ņāØĒĢ£ļŗż.8) Ļ│© ņĀäņØ┤ļŖö Ļ│ĀļĀ╣ņØś ĒÖśņ×ÉņŚÉņä£ ļŹö ņ×ÉņŻ╝ ļ░£ņāØĒĢśļ®░, ļŗżļ░£ņä▒ Ļ│© ņĀäņØ┤ļŖö ļŗ©ņØ╝ Ļ│© ņĀäņØ┤ļ│┤ļŗż ņ×ÉņŻ╝ Ļ┤Ćņ░░ļÉ£ļŗż.9) Ļ░æņāüņäĀ ņŚ¼ĒżņĢö ņżæ Ļ│© ņĀäņØ┤ļŖö 27.8% ļ╣äņ£©ņŚÉņä£ ļ│┤ņØ┤ļ®░,10) Ļ░æņāüņäĀ ņŚ¼ĒżņĢöņØś Ļ│© ņĀäņØ┤ ņżæ ļæÉĻ░£Ļ│© ņĀäņØ┤ļŖö 27%ņØś ļ╣äņ£©ņØä ļ│┤ņØĖļŗż.10,11) Nagamine ļō▒12)ņØś ļ│┤Ļ│ĀņŚÉņä£ 473Ļ▒┤ņØś Ļ░æņāüņäĀ ņĢö ņ”ØļĪĆ ņżæ 9Ļ▒┤ņØś Ļ░æņāüņäĀ ņŚ¼ĒżņĢöņØś ļæÉĻ░£Ļ│© ņĀäņØ┤Ļ░Ć ļ│┤Ļ│ĀļÉśņŚłĻ│Ā, ĒøäļæÉĻ│©, ļæÉņĀĢ-ĒøäļæÉĻ│©, ņĀäļæÉĻ│©, ņĀäļæÉ-ļæÉņĀĢĻ│©, ļæÉĻ░£ņĀĆ, ļæÉņĀĢĻ│© ņł£ņä£ņØś ļ╣łļÅäļź╝ ļ│┤ņØ┤ļ®░, ļīĆĻ░£ ĒøäļæÉļČĆņØś ļŗ©ļŗ©ĒĢśņ¦Ć ņĢŖņØĆ ļ¼┤ĒåĄņØś ļŹ®ņØ┤ļĪ£ ļ░£Ļ▓¼ļÉśņŚłļŗż. Varadarajan ļō▒13)ņØĆ Ļ░æņāüņäĀ ņŚ¼ĒżņĢöņØś ņĢłļ®┤Ļ│© ņĀäņØ┤ 34Ļ▒┤ņØś ņ”ØļĪĆļź╝ ļ│┤Ļ│ĀĒĢśņśĆĻ│Ā, ņØ┤ņżæ ņĢłņÖĆĻ│©ļĪ£ ņĀäņØ┤ļÉ£ Ļ▓ĮņÜ░ļŖö 4ļĪĆņśĆļŗż.
Jun Shen ļō▒14)ņØĆ Ļ░æņāüņäĀ ņŚ¼ĒżņĢöņØś ļæÉĻ░£Ļ│© ņĀäņØ┤ļź╝ ļ│┤ņØĖ ĒÖśņ×É ņ”ØļĪĆ ņżæ ļé┤ņøÉ 3Ļ░£ņøö ņĀäļČĆĒä░ ņ¦ĆņåŹļÉ£ ņÜ░ņĖĪ ņØ┤ļ¦łņØś ļ¼┤ĒåĄņä▒ ņóģļ¼╝Ļ│╝ ļé┤ņøÉ 7Ļ░£ņøöņĀäļČĆĒä░ ņ¦ĆņåŹļÉ£ ņÜ░ņĢłņØś ņŗ£ņĢ╝ ĒØÉļ”╝ņØä ņŻ╝ņåīļĪ£ ļé┤ņøÉĒĢ£ 67ņäĖ ļé©ņ×É ĒÖśņ×Éļź╝ ļ│┤Ļ│ĀĒĢ£ ļ░ö ņ׳ļŗż. ņśüņāü Ļ▓Ćņé¼ņāüņŚÉņä£ ņÜ░ņĖĪ ņĢłņÖĆ ļ░Å ņĀäļæÉļÅÖņØś Ļ│©ņ£ĄĒĢ┤ņä▒ņØś ļŗ©ņØ╝ ņóģļ¼╝ņØ┤ ĒÖĢņØĖļÉśņ¢┤ ņłśļ¦ēņóģ ļśÉļŖö ņĀäņØ┤ņä▒ ņĢöņóģņØ┤ ņØśņŗ¼ļÉśņ¢┤, ņÜ░ņĖĪ ņĀäļæÉļÅÖ Ļ░£ļæÉņłĀļĪ£ ņóģļ¼╝ ņĀ£Ļ▒░ Ēøä ņĪ░ņ¦üĻ▓Ćņé¼ņŚÉņä£ Ļ░æņāüņäĀ ņŚ¼ĒżņĢöņØś ņĀäņØ┤ļĪ£ ĒÖĢņØĖļÉśņŚłņ£╝ļéś, Ļ▓░ĻĄŁ ņłśņłĀ 20Ļ░£ņøö Ēøä Ļ▓ĮļČĆ ļ░Å ņóģĻ▓®ļÅÖņØś ļŗżļ░£ņä▒ ņĀäņŗĀ ņĀäņØ┤ļĪ£ ņé¼ļ¦ØĒĢśņśĆļŗż. ļ│Ė ņ”ØļĪĆņÖĆ Ļ░ÖņØ┤ Ļ│ĀļĀ╣ņØś ĒÖśņ×ÉņŚÉņä£ Ļ░æņāüņäĀ ņŚ¼ĒżņĢöņØś ņĀäņØ┤ļĪ£ ļŗ©ņØ╝ņä▒ ņĢłņÖĆ Ļ│©ļ│æļ│ĆņØ┤ ļ│┤ņśĆĻ│Ā, ņĀäņŗĀ ņĀäņØ┤ļĪ£ ļ░£ņĀäĒĢ£ ņ”ØļĪĆņØ┤ļŗż. Jun ShenņØś ņ”ØļĪĆļź╝ ĒżĒĢ©ĒĢśņŚ¼ Ēśäņ×¼Ļ╣īņ¦Ć Ļ░æņāüņäĀ ņŚ¼ĒżņĢöņØś ņĢłņÖĆĻ│© ņĀäņØ┤ļŖö ļŗ© 11Ļ▒┤ ļ│┤Ļ│ĀĻ░Ć ļÉśņŚłņØä ņĀĢļÅäļĪ£,13-18) ļ¦żņÜ░ ļō£ļ¼╝Ļ▓ī Ļ┤Ćņ░░ļÉ£ļŗż.
Ļ░æņāüņäĀ ņĢöņØś Ļ│© ņĀäņØ┤ņŚÉ ļīĆĒĢ£ ņ╣śļŻīļŖö ļ░®ņé¼ņäĀ ņÜöņśżļō£ ņ╣śļŻī, ņłśņłĀ, ņÖĖļČĆ ņĪ░ņé¼ ļ░®ņé¼ņäĀ ņ╣śļŻī ļ░Å ĒĢŁņĢö ĒÖöĒĢÖ ņÜöļ▓ĢņØ┤ ņ׳ļŗż. Ļ│© ņĀäņØ┤ņŚÉ ļŗ©ļÅģ ļ░®ņé¼ņä▒ ņÜöņśżļō£ ņ╣śļŻīļŖö ņĀĆĒĢŁņä▒ņØä ļ│┤ņØ┤ļŖö Ļ▓ĮņÜ░Ļ░Ć ļ¦ÄņĢäņä£ ļīĆļČĆļČä ļ│æĒĢ® ņÜöļ▓ĢņØ┤ ĒĢäņÜöĒĢśņŚ¼, ņłśņłĀņØ┤ Ļ░ĆļŖźĒĢ£ Ļ▓ĮņÜ░ņŚÉļŖö Ļ│© ņĀäņØ┤ ļ│æļ│Ć ņĀłņĀ£ņłĀņØ┤ ņČöņ▓£ļÉ£ļŗż.19) Ļ│© ņĀäņØ┤ ļ│æļ│Ć ņĀłņĀ£ņłĀņØĆ Ļ│© ņĀäņØ┤ ļČĆņ£ä ņĀłņĀ£ņŚ░ ļ░Å ļŗżļźĖ ņĀäņØ┤ ļČĆņ£äņŚÉ ļīĆĒĢ£ ļ░®ņé¼ņä▒ ņÜöņśżļō£ ņ╣śļŻīņØś ĒÜ©Ļ│╝ļź╝ ļåÆņØ╝ ņłś ņ׳ĻĖ░ ļĢīļ¼ĖņØ┤ļŗż.6,20) ļŗżņä» ļČĆņ£ä ņØ┤ĒĢśņØś Ļ│© ņĀäņØ┤ ļ│æļ│ĆņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░, Ļ│© ņĀäņØ┤ ļ│æļ│Ć ņĀ£Ļ▒░ ņłśņłĀņØä ĒåĄĒĢ┤ ņāØņĪ┤ļźĀņØä ļåÆņØ┤Ļ│Ā ņéČņØś ņ¦łņØä Ļ░£ņäĀņŗ£Ēé¼ ņłś ņ׳ļŗżļŖö ļ│┤Ļ│ĀĻ░Ć ņ׳ņ¢┤,9) ņłśņłĀņĀü ņĀłņĀ£Ļ░Ć Ļ░ĆļŖźĒĢ£ Ļ│© ņĀäņØ┤ ļ│æļ│ĆņŚÉ ļīĆĒĢ┤ņä£ļŖö ņĀüĻĘ╣ņĀüņØĖ ņłśņłĀņØ┤ ĒĢäņÜöĒĢśļŗż.19,21) ņÖĖļČĆ ļ░®ņé¼ņäĀ ņ╣śļŻīļŖö ļ░®ņé¼ņä▒ ņÜöņśżļō£ ņ╣śļŻīņŚÉ ļ░śņØæņØ┤ ņŚåļŖö Ļ▓ĮņÜ░ ņĀüņÜ® Ļ░ĆļŖźĒĢśĻ│Ā, ņ×¼ļ░£ļźĀĻ│╝ Ļ│© ņĀäņØ┤ ļČĆņ£äņØś ĒåĄņ”ØņØä ņØ╝ļČĆ ļé«ņČ£ ņłś ņ׳ļŗżĻ│Ā ļ│┤Ļ│ĀļÉśņŚłļŗż.19) Ļ│╝Ļ▒░ ĒĢŁņĢö ĒÖöĒĢÖ ņÜöļ▓ĢņØĆ etoposide, carboplatin, cisplatin, methotrexate, adriamycin, doxorubicin ļŗ©ļÅģ ņÜöļ▓ĢņØ┤ļéś, adriamycin, bleomycin, vincristine ļ│æĒĢ® ņÜöļ▓Ģ, adriamycin, bleomycin, cisplatin ļ│æĒĢ® ņÜöļ▓Ģ Ēś╣ņØĆ doxorubicin, cisplatin ļ│æĒĢ® ņÜöļ▓Ģ ļō▒ ļŗżņ¢æĒĢ£ ņĢĮņĀ£Ļ░Ć ņŗ£ļÅäļÉśņŚłņ¦Ćļ¦ī ņ╣śļŻī ņä▒Ļ│╝Ļ░Ć ņóŗņ¦Ć ļ¬╗ĒĢśņśĆĻ│Ā,22-24) ņĄ£ĻĘ╝ Ēæ£ņĀü ĒĢŁņĢöņ╣śļŻīņĀ£ lenvatinibņØ┤ ļ¼┤ņ¦äĒ¢ēņāØņĪ┤(progression-free survival)ņŚÉ ņä▒Ļ│╝Ļ░Ć ņ׳ļŗżļŖö ļ│┤Ļ│ĀĻ░Ć ņ׳ļŗż.25)
ļ│Ė ņ”ØļĪĆņŚÉņä£ļŖö ņłśņłĀ ņĀä Ļ▓Ćņé¼ņŚÉņä£ Ļ░æņāüņäĀ ņÜ░ņŚĮņØś Ļ▒░ļīĆ ņóģļ¼╝Ļ│╝ ĒĢ©Ļ╗ś ņóīņĖĪ ņĢłņÖĆņØś ļŗ©ņØ╝ ņóģļ¼╝ņØ┤ ļ░£Ļ▓¼ļÉśņŚłļŗż. ņóīņĖĪ ņĢłņÖĆņØś ļŗ©ņØ╝ ņóģļ¼╝ņØĆ ņłśņłĀ ņĀä Ļ▓Ćņé¼ņŚÉņä£ ļ”╝Ēöäņóģņ£╝ļĪ£ ņØśņŗ¼ļÉśņŚłņ£╝ļéś, ņóīņĖĪ ņĢłņÖĆĻ│© ļ│æļ│Ć ņĀłņĀ£ņłĀ Ēøä ņĪ░ņ¦üĻ▓Ćņé¼ņŚÉņä£ Ļ░æņāüņäĀ ņŚ¼ĒżņĢöņØś ņĀäņØ┤ļĪ£ ĒÖĢņØĖļÉśņŚłĻ│Ā, ņØ┤Ēøä ņśüņāüĻ▓Ćņé¼ņŚÉņä£ ļŗżļ░£ņä▒ Ļ│© ņĀäņØ┤ ļ░Å ņĀäņŗĀ ņĀäņØ┤Ļ░Ć ĒÖĢņØĖļÉśņŚłļŗż.
ņĀĆņ×ÉļōżņØĆ ļ│Ė ņ”ØļĪĆļź╝ ĒåĄĒĢśņŚ¼ Ļ│ĀļĀ╣ņØś ĒÖśņ×ÉĻ░Ć Ļ░æņāüņäĀ Ļ▒░ļīĆ ņóģļ¼╝Ļ│╝ ĒĢ©Ļ╗ś ņĢłņÖĆņØś ļŗ©ņØ╝ ņóģļ¼╝ņØä ļÅÖļ░śĒĢ£ Ļ▓ĮņÜ░, Ļ░æņāüņäĀ ņŚ¼ĒżņĢöņØś ņĢłņÖĆĻ│© ņĀäņØ┤ņØś ļ░£ļ│æļźĀņØĆ ļé«ņ¦Ćļ¦ī, ĻĘĖ Ļ░ĆļŖźņä▒ļÅä ņČ®ļČäĒ׳ Ļ│ĀļĀżĒĢ┤ņĢ╝ ĒĢ©ņØä Ļ▓ĮĒŚśĒĢśņśĆļŗż. ļśÉĒĢ£ ļ│Ė ņ”ØļĪĆņŚÉņä£ Ļ▓░Ļ│╝ņĀüņ£╝ļĪ£ ĒÖśņ×ÉņØś Ļ░æņāüņäĀ ņŚ¼ĒżņĢöņØś ņĀäņŗĀ ņĀäņØ┤Ļ░Ć ĒÖĢņØĖļÉśņŚłĻĖ░ņŚÉ, ņĢłņÖĆņØś ļŗ©ņØ╝ ņóģļ¼╝ņØĆ Ļ░æņāüņäĀ ņĢöņØś Ļ│© ņĀäņØ┤ņÖĆ ļŹöļČłņ¢┤ ņĀäņŗĀ ņĀäņØ┤ņØś ņ×äņāüņĀü ņ¦ĢĒøäļĪ£ ņØśņŗ¼ĒĢśĻ│Ā ņĀüĻĘ╣ņĀüņØĖ Ļ▓Ćņé¼ ļ░Å ņ╣śļŻīļź╝ Ļ│ĀļĀżĒĢ┤ņĢ╝ ĒĢĀ Ļ▓āņØ┤ļŗż.




