

서론
VHL 증후군은 상염색체 우성으로 유전되는 질환으로 서양에서의 보고에 의하면 유병률은 35,000에서 40,000명 중 한명 정도로 특징적인 병변은 망막 혈관모세포종(hemangioblastoma), 소뇌와 척수의 혈관모세포종, 신장과 췌장의 낭종 및 암종, 부신의 갈색세포종(pheochromocytoma), 부고환의 낭선종(epididymal cystadenoma), 내림프낭종(endolymphatic sac tumor), 간과 비장 및 폐의 낭종 등과 같은 다양한 장기에 다양한 양성 및 악성 종양을 유발하는 복합 증후군이다.1)
그 중 혈관모세포종은 VHL 증후군에서 가장 흔한 병변으로 뇌와 척수, 망막 등 신경계에서 발생하는 혈관종의 한 종류이고, VHL 환자에서 일생 동안 60-80%에서 발생하고,2) 혈관모세포종의 30%는 VHL 증후군과 관련있을 정도로 밀접한 관련이 있다.3) 하지만 VHL 증후군에서 위에서 언급한 장기 외의 침범은 드물고 나타난다면 혈관종 또는 낭종 등 양성 종양의 형태로 나타나며, 비강을 침범한 종양에 관련해서는 VHL 증후군에서 가장 흔한 악성 종양인 신세포암(renal cell carcinoma)의 전이와 소낭성선종(microcystic adenoma)과 함께 최근들어 sinonasal renal cell-like adenocarcinoma (SNRCLA) 등이 일부 보고되고 있다.4,5)
저자들은 VHL 증후군 환자에서 비강 내에 발생한 혈관종 1예를 치험하였기에 문헌고찰과 함께 보고하고자 한다.
증례
환자는 26세 여성으로 우연히 췌장 및 우측 부신 종양이 발견되어 유전자 검사상 VHL syndrome으로 진단받은 환자로 2022년 3월 우측 부신절제술, 2022년 5월 유문부 보존 췌두부십이지장절제술(Pylorous-preserving pacnreaticoduodenectomy, PPPD) 시행 받고 병리조직검사에서 부신의 갈색세포종(Pheochromocytoma), 췌장 신경내분비종양(pancreatic neuroendocrine tumor) 소견을 보였다.
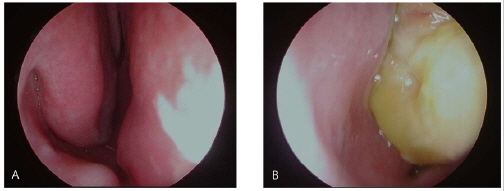
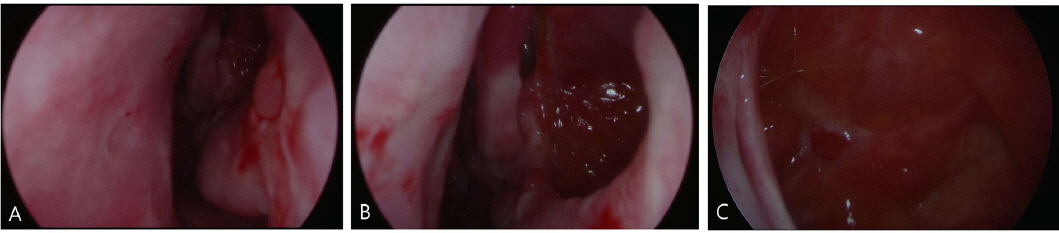
환자는 2023년 3월경 4개월 전부터 악화되는 좌측 비폐색, 비루로 내원하였고 이전 반복적인 비출혈, 코 수술력 및 안면 외상력은 없었으며 비내시경 검사상 좌측 비강을 가득 채우는 연한 노란색의 종양과 점액성 비루가 확인되었다(Fig. 1). 상기 종양에 대하여 외래에서 펀치 생검(punch biopsy)을 시행하였으나 조직병리검사 결과 만성 염증을 동반한 괴사 조직만이 관찰되었고 시술 후 출혈이 심하였다.
Fig. 1
Preoperative nasal endoscopic findings. (A) Right side of nasal cavity, (B) left side of nasal cavity with expansile yellowish mass.
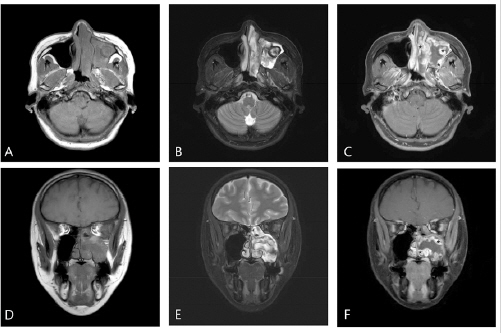
조영제를 사용한 부비동 전산화단층촬영(paranasal sinus computed tomography, PNS CT)에서 좌측 전두동, 사골동, 상악동 및 비강에 연조직 음영이 보이며 상악동에서는 비균질하게 조영되고 상악동의 개구부(maxillary sinus ostium)가 확장된 양상이 관찰되었고 골조직의 파괴는 없었다(Fig. 2). 추가로 시행한 부비동 자기공명영상(paranasal sinus magnetic resonance imaging, PNS MRI)의 T1 강조영상에서 좌측 상악동과 비강에 비균질한 저강도 신호를 보이는 종괴가 가돌리늄(gadolinium) 조영제에 일부 조영증강되는 양상을 보였고, T2 강조영상에서는 비균질한 고강도 신호를 보였다(Fig. 3).
Fig. 2
Preoperative computed tomography (CT). (A) Axial, (B) coronal, (C) enhanced axial, (D) enhanced coronal PNS CT show a large soft-tissue opacity occupying the left maxillary sinus with multifocal heterogenous enhancement and widening the maxillary ostium.
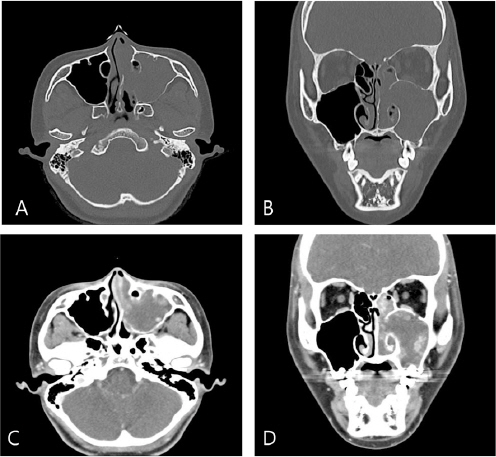
Fig. 3
Preoperative magnetic resonance imaging (MRI), (A-C) axial and (D-F) coronal image. There are heterogenous intensities on left nasal cavity and maxillary sinus which are (A, D) low intensity on T1-weighed image, (B, E) high signal on T2-weighted image and (C, F) enhancing after gadolinium enhancement (*) on T1-weighted image.
이에 대해 상악동 기원의 반전성 유두종(inverted papilloma), 악성 종양, 혈관종 등의 가능성을 고려하였고 종양의 완전 제거 및 출혈의 용이한 조절을 위해 전누골와 접근법(prelacrimal recess approach)을 이용한 내시경하 상악동 종양 절제술 및 내시경하 부비동 수술을 시행하였다.
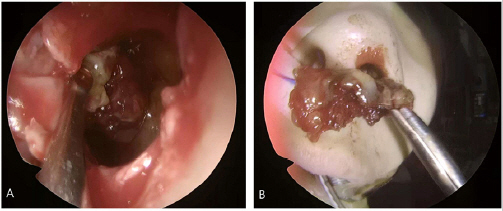
시야 확보를 위해 좌측 비강 내의 종양을 먼저 절제한 후 중비도 개창술을 시행하여 상악동 내 종양을 확인 및 일부 제거하였고, 하비갑개의 전부착부에서 수직 절개를 가하고 하비도 외측벽을 제거 후 상악동 내부로 접근하자 울퉁불퉁한 윤곽에 황갈색과 흰색, 붉은색이 혼재된 양상의 종양이 상악동의 후벽에 부착되어 있었으며 종양의 일부를 절제하여 동결절편검사를 시행하였으나 염증, 섬유화, 출혈 소견만이 확인되었다. 상악동내 종양을 완전히 제거하고 부착부위는 다이아몬드 버로 갈아낸 후 동결절편검사를 시행하여 잔여 병변이 없음을 확인하였다. 이후 하비갑개 점막을 원래 자리에 위치시킨 후 봉합하여 수술을 마무리 하였다. 수술 중 출혈은 심하지 않았으며, 비루관(nasolacrimal duct)과 이상구(pyriform aperture)는 보존하였다(Fig. 4).
Fig. 4
Intraoperative endoscopic findings. (A) A mass attached to maxillary sinus posterior wall is visible through prelacrimalrecess approach. (B) The mass showed mixture of yellow-brown, white and red colors and had irregular surface.
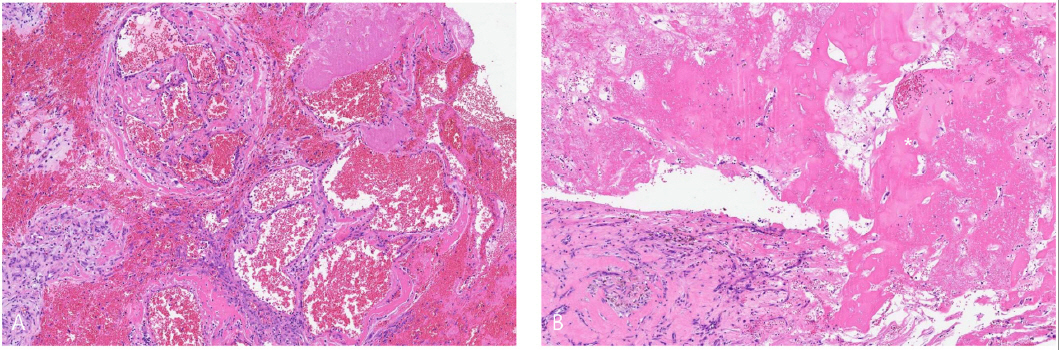
환자는 수술 후 이틀째에 특별한 합병증 없이 퇴원하였고, 조직병리검사상 점막하 조직 내로 확장된 혈관들이 모여있는 소견을 보여(Fig. 5A) 해면상혈관종으로 최종 진단되었고, 주변으로 섬유화(fibrosis)와 헤모시데린 색소(hemosiderin pigment)가 침착되어 있는 소견(Fig. 5B)이 보여 혈관종의 출혈로 이차적으로 발생한 것으로 추정되는 기질화혈관종이 동반되어있었다. 환자는 6개월 째 외래에서 추적관찰 중에 있으며 비내시경(Fig. 6) 및 전산화단층촬영(Fig. 7)에서 재발 및 합병증의 소견은 보이지 않았다.
Fig. 5
Light microscopic finding of excised mass shows (A) aggregated dilated vessels with hemorrhage and fibrinoid materials (H&E, x100), representing cavernous hemangioma and (B) diffuse fibrosis and hemosiderin pigments deposition (H&E, x100), accompanying organized hematoma.

고찰
VHL 증후군은 다양한 장기에서 양성 및 악성 종양을 유발하는 복합 증후군으로 진단기준은 저자에 따라 약간의 차이는 있으나, VHL 증후군의 가족력이 있는 경우 특징적인 종양성 병변을 한가지 이상, 가족력이 없는 경우에는 두가지 이상을 가지는 경우 임상적 진단이 가능하고 확진은 유전자 검사에 의해 이루어진다(Table 1)6).
Table 1
Diagnostic criteria for von Hippel-Lindau syndrome
이 중 내림프낭종과 같이 VHL 증후군에서 호발하지만 진단기준에는 포함되지 않는 종양성 병변들도 있으나, 비부비강에서의 침범은 드물고 VHL 증후군에서 가장 흔한 암인 투명세포형 신세포암(clear cell renal cell carcinoma, ccRCC)의 전이나7) 이와 비슷한 조직학적 특징을 가지는 비강에서 원발한 악성종양인 sinonasal renal cell-like adenocarcinoma (SNRCLA) 예가 최근 보고되고 있다.4)
혈관종은 주로 선천적 요인으로 발생하는 양성 종양으로 50% 이상이 두경부 영역에서 발생하는 것으로 알려져 있는데, 전체의 95%가 6개월 이내에 발생되고 1세 이후에는 자연 퇴화하는 경향을 보여 5세 이후에는 1.6%만이 남아있는 것으로 알려져 있다.8) 분류는 소아형, 성인형으로 분류하거나 조직병리검사상 혈관의 크기에 따라 해면형, 모세혈관형 및 혼합형으로 분류하기도 한다. 소아에서는 모세혈관형이 많으나, 성인에서는 해면형이 더 많다. 이는 상대적으로 해면형의 퇴화 비율이 적기 때문이다.9) 비부비강내 혈관종은 비중격이나 비전정에서 호발하고, 임상양상으로는 비폐색, 비출혈이 흔하며 대부분 적색의 과혈관증식성 종양 형태로 관찰된다.10) 진단은 병력청취, 신체검사, 전산화단층촬영, 자기공명영상, 혈관조영검사 등이 활용될 수 있고 확진은 병리조직검사로 이루어지게 되는데 감별해야 할 질환으로는 반전성 유두종, 후각 신경아세포종(olfactory neuroblastoma), 편평상피세포암(squamous cell carcinoma), 신세포암의 전이 등이 있다.11) 치료는 추적 관찰로부터 수술까지 다양하지만, 성인에서 발생한 경우에는 자연관해가 드물기 때문에 적극적인 치료가 권유된다. 수술적 치료시 다량의 출혈위험성이 있으므로 술전 평가가 중요하며 CT에서 과혈관성을 시사하는 소견을 보이거나 혈관종이 큰 경우에는 수술시 출혈을 줄이기 위해 혈관조영술을 시행하여 혈관 분포를 확인한 뒤 색전술을 시행할 수도 있다.12) 중비도 개창술과 함께 전누골와 접근법을 시행하는 경우 Caldwell-Luc 접근법이나 내측 상악동 절제술(medial maxillectomy)과 달리 코눈물관이나 하비갑개의 손상 없이 상악동의 완전한 시야를 얻을 수 있다. 본 증례의 경우 종물이 상악동 내에 위치하고 있고 전누골와 접근법과 중비도 개창술로 충분한 시야로 색전술을 시행하지 않더라도 병변의 완전한 제거와 술 중 출혈을 조절할 수 있을 것으로 판단되어 시행하지 않았다.
혈관종은 두경부에서는 비교적 흔한 종양이나 성인에서 발생하는 경우가 흔하지 않고 상악동에서 발생한 경우는 더욱 드물어 국내외로 보고된 예가 적고 VHL 증후군과 연관된 경우는 보고된 적이 없다.
VHL 증후군에서는 망막 및 소뇌의 혈관모세포종이 가장 흔한 병변으로 이외에도 신장의 낭종이나 악성 종양, 부신의 갈색세포종, 췌장의 낭종이나 종양, 부고환의 낭선종, 내림프낭종등 여러 장기에서 양성 및 악성 종양을 유발하지만1), 이외 다른 장기들의 침범은 드물고 발생한다면 혈관종이나 낭종의 형태로 발견된다13)(Table 2)1). 본 증례 환자의 경우는 이전 VHL 증후군 진단 후 안과 검진 및 brain MRI상 망막이상이나 뇌실질에 병변은 발견되지 않았으며, 부신의 갈색세포종, 췌장의 신경내분비종양, 비강의 해면상 혈관종이 발견되었다.
Table 2
Possible lesions of central nervous system and intravisceral organ in von Hippel-Lindau syndrome
VHL 증후군은 3번 상염색체의 단완(short arm)에 있는 종양 억제 유전자(tumor suppressor gene)인 VHL유전자의 생식세포 돌연변이(germline mutation)에 의해 발생한다.14) 이 유전자의 변이는 저산소증 유도 인자 1α와 2α (Hypoxia-inducible factor 1α and 2α, HIF 1α and 2α)를 안정화(stabilization)시키는데, 이 전사인자(transcription factor)들은 정상적인 산소 농도에서 불안정한 상태로 저산소 환경에서 안정화되면 vascular endothelial growth factor (VEGF)의 발현(expression)을 증가시켜 혈관신생(angiogenesis)을 촉진하는 역할을 한다.15) 즉, VHL유전자의 변이는 정상적인 산소농도에서도 VEGF의 과발현을 유발하고, 이는 혈관종의 병태생리에 중요한 역할을 하는 것으로 생각된다.
본 증례의 경우 다양한 장기에 종양을 유발하는 증후군을 가진 환자의 편측에서 비교적 급성의 경과를 가지며, 외래에서 출혈 경향성을 보이는 종양을 보이는 임상소견으로 혈관종, 반전성 유두종과 SNRCLA 등의 악성 종양의 가능성까지 고려하였고, 전누골와 접근법과 중비도 상악동 개방술을 통해 수술적 치료를 시행하였고 많은 출혈 없이 용이하게 병변을 제거 후 해면상 혈관종이 진단되었다.
저자들은 희귀질환인 VHL 증후군 환자에서 동반된 부비동에서는 발생이 드문 혈관종을 성공적으로 치험하였으며, 이에 문헌고찰과 함께 보고하고자 한다.




