

ņä£ļĪĀ
ņ╣śņä▒ Ļ░üĒÖöņä▒ ļéŁņóģ(odontogenic keratocyst)ņØĆ ņĢģĻ│©ņØś ļéŁņóģ ņżæ 3-11%ļź╝ ņ░©ņ¦ĆĒĢśļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ņ£╝ļ®░, ņ╣śņ▓┤(dental lamina)ņØś ņ×öņĪ┤ņäĖĒż(cell rest)ļĪ£ļČĆĒä░ ĻĖ░ņøÉĒĢ£ļŗż.1,2) ņāüņĢģļ│┤ļŗżļŖö ĒĢśņĢģņŚÉ ļŹö ņל ņāØĻĖ░ļ®░, ĒĢśņĢģ ņĀ£ 3ļīĆĻĄ¼ņ╣ś ļ░Å ņĀ£ 1,2 ļīĆĻĄ¼ņ╣ś ņł£ņ£╝ļĪ£ ĒśĖļ░£ĒĢśĻ│Ā ņāüņĢģņØĆ ņĀ£ 3 ļīĆĻĄ¼ņ╣śĻ░Ć Ļ░Ćņן ĒØöĒĢ£ ļČĆņ£äļĪ£ ļ│┤Ļ│ĀļÉśĻ│Ā ņ׳ļŗż.
ļ╝łņŚÉ ņāØĻĖ░ļŖö ĒÄĖĒÅēņäĖĒżņĢöņóģņØĆ ļ¦żņÜ░ ļō£ļ¼╝ļ®░, ļīĆļČĆļČäņØĆ ņ×öļźś ļéŁņóģ(residual cyst), ļ¦żļ¬░ ņ╣śņĢä ļéŁņóģ(dentigerous cyst), ņ╣śņä▒ Ļ░üĒÖöņä▒ ļéŁņóģĻ│╝ Ļ░ÖņØĆ ņ╣śņä▒ ļéŁņóģņŚÉņä£ ļ░£ņāØĒĢśĻ│Ā, ņØ┤ļŖö ņ╣śņä▒ ļéŁņóģņŚÉņä£ ĻĖ░ņøÉĒĢ£ ņøÉļ░£ņä▒ Ļ│©ļé┤ ĒÄĖĒÅēņāüĒö╝ņäĖĒż ņĢöņóģ(Primary intraosseous squamous cell carcinoma ex odontogenic cyst, PIOSCC ex odontogenic cyst)ņ£╝ļĪ£ ĒåĄņ╣ŁĒĢśņŚ¼ ļČłļ”░ļŗż. ņØ┤ ļéŁņóģ ņżæ, ņ╣śņä▒ Ļ░üĒÖöņä▒ ļéŁņóģņØś ņäĖĒżĻ░Ć ļŗżļźĖ ņ╣śņä▒ ļéŁņóģņŚÉ ļ╣äĒĢ┤ ļŹö ļåÆņØĆ ņ▓┤ņäĖĒż ļČäņŚ┤(mitotic activity)ļź╝ Ļ░Ćņ¦ĆĻ│Ā ņ׳ņ¢┤ ĒÄĖĒÅēņäĖĒżņĢöņóģņ£╝ļĪ£ ņĀäĒÖś Ļ░ĆļŖźņä▒ņØ┤ ļåÆņ¦Ćļ¦ī, ņØ┤ļ¦łņĀĆļÅä ļō£ļ¼╝ļŗż.3)
ņĀĆņ×ÉļōżņØĆ ņ╣śņä▒ Ļ░üĒÖöņä▒ ļéŁņóģņ£╝ļĪ£ ĒāĆļ│æņøÉņŚÉņä£ ņłśņłĀ Ēøä ļ░£Ļ▓¼ļÉ£ ņĢģņä▒ ņóģņ¢æņ£╝ļĪ£ ļé┤ņøÉĒĢ£ ĒÖśņ×ÉņŚÉņä£, ĒÄĖĒÅēņäĖĒżņĢöņóģņØä ĒÖĢņØĖĒĢśņśĆĻ│Ā ĻĘ╝ņ╣śņĀü ņłśņłĀļĪ£ņä£ ņ╣śļŻīļź╝ ĒĢ£ ļ╣äĻĄÉņĀü ļō£ļ¼Ė ņ”ØļĪĆļź╝ Ļ▓ĮĒŚśĒĢśņśĆĻĖ░ņŚÉ ļ¼ĖĒŚī Ļ│Āņ░░Ļ│╝ ĒĢ©Ļ╗ś ļ│┤Ļ│ĀĒĢśļŖö ļ░öņØ┤ļŗż.
ņ”ØļĪĆ
63ņäĖ ļé©ņ×ÉĒÖśņ×ÉĻ░Ć ņŗØņé¼ ņżæ ņÜ░ņŚ░Ē׳ ņÜ░ņĖĪ ĒĢśņĢģ ņ¢┤ĻĖłļŗłĻ░Ć Ļ╣©ņĀĖ ĻĘ╝ņ▓ś ņ╣śĻ│╝ļ│æņøÉ ļé┤ņøÉĒĢśņŚ¼ ņÜ░ņĖĪ ĒĢśņĢģ ņĀ£3ļīĆĻĄ¼ņ╣ś ņĢäļל ļ¼╝Ēś╣ ņåīĻ▓¼ņØ┤ ĒÖĢņØĖļÉśņŚłļŗż. ĒĢ┤ļŗ╣ ņ╣śņĢäņÖĆ Ļ┤ĆļĀ©ĒĢśņŚ¼ Ļ│╝Ļ▒░ņŚÉ ņ”ØņāüņØ┤ ņ׳Ļ▒░ļéś ņ╣śļŻīĒĢ£ ļ│æļĀźņØĆ ņŚåņŚłļŗż. ņØ┤ņŚÉ ĻĘ╝ņ▓ś ļīĆĒĢÖļ│æņøÉ ļé┤ņøÉĒĢśņŚ¼ ļ¦żļ│Ą ņ╣śņĢä ņåīĻ▓¼Ļ│╝ ĒĢ©Ļ╗ś ņÜ░ņĖĪ ĒĢśņĢģņØś Ļ░ÉņŚ╝ņä▒ ņ╣śņä▒ Ļ░üĒÖöļéŁ ņ¦äļŗ©ņ£╝ļĪ£ ņĀäņŗĀļ¦łņĘ©ĒĢś ļéŁņóģ ņĀüņČ£ņłĀ ļ░Å ĒĢ┤ļŗ╣ ņ╣śņĢä ļ░£ņ╣ś ņłśņłĀĒĢśņśĆĻ│Ā, ņĪ░ņ¦üĻ▓Ćņé¼ Ļ▓░Ļ│╝ ĒĢśņĢģĻ│©ļé┤ ņĢöņóģ ņåīĻ▓¼ļ│┤ņŚ¼ ļ│ĖņøÉ ņØ┤ļ╣äņØĖĒøäĻ│╝ ņÖĖļלļĪ£ ļé┤ņøÉĒĢśņśĆļŗż. ĻĖ░ņĀĆ ņ¦łĒÖśņ£╝ļĪ£ņä£ ļŗ╣ļć©ņÖĆ Ļ│Āņ¦ĆĒśłņ”ØņŚÉ ļīĆĒĢ£ Ļ▓ĮĻĄ¼ņĢĮ ļ│ĄņÜ®ļĀź ņÖĖņŚÉļŖö ĒŖ╣ņØ┤ņé¼ĒĢŁņØ┤ ņŚåņŚłļŗż.
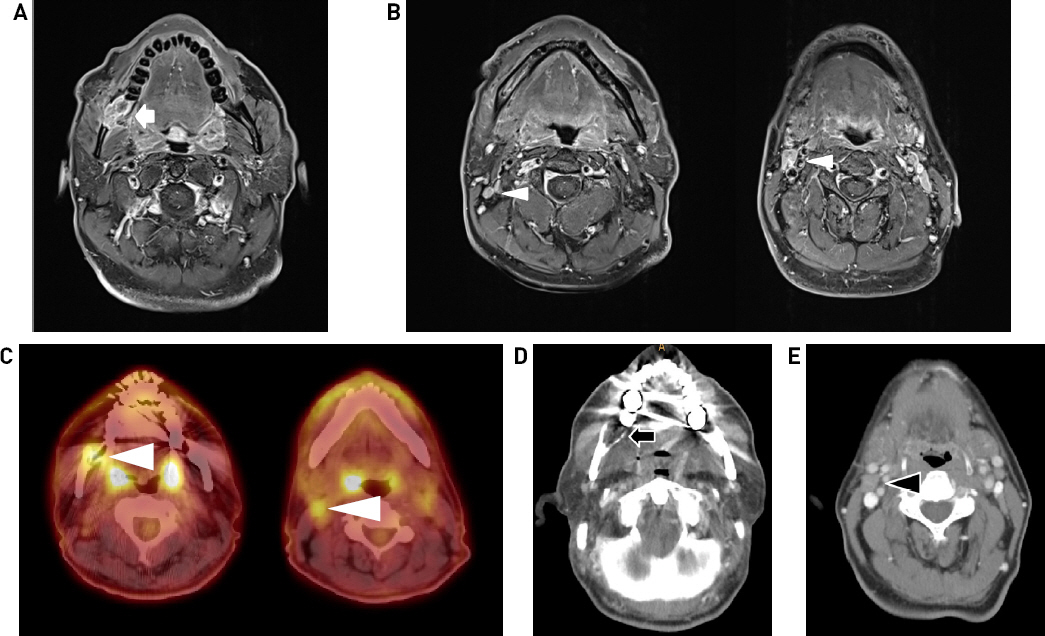
ĒÖśņ×ÉļŖö ļé┤ņøÉ ļŗ╣ņŗ£ ĒŖ╣ņØ┤ ĒśĖņåī ņ”Øņāü ņŚåņŚłņ£╝ļ®░, ņŗĀņ▓┤ ņ¦äņ░░ņāü ĻĄ¼Ļ░Ģļé┤ ņĀÉļ¦ē ļ│æļ│ĆņØ┤ļéś ņóģļ¼╝ ļō▒ ĒŖ╣ņØ┤ņåīĻ▓¼ ņŚåņŚłĻ│Ā, Ļ▓ĮļČĆņŚÉ ņ┤ēņ¦ĆļÉśļŖö ņóģļ¼╝ņØĆ ņŚåņŚłļŗż(Fig. 1). ĒāĆļīĆĒĢÖļ│æņøÉņŚÉņä£ ļŗ╣ņŗ£ ņłśņłĀ Ēøä ņŗ£Ē¢ēĒĢ£ ņśüņāüĻ▓Ćņé¼ņāü, ņ×ÉĻĖ░Ļ│Ąļ¬ģņśüņāüņŚÉņä£ ņÜ░ņĖĪ ĒĢśņĢģĻ░üņŚÉ Ļ│© ļ»Ėļ×ĆņØä ļÅÖļ░śĒĢśļŖö ņןĻ▓Į 2.3cm Ēü¼ĻĖ░ņØś ņóģļ¼╝ ļ░Å ņÜ░ņĖĪ Ļ▓ĮļČĆ ļĀłļ▓© IIņŚÉ ļŗżļ░£ņä▒ ļ”╝ĒöäņĀł ļ╣äļīĆņåīĻ▓¼ ļ│┤ņśĆļŗż(Figs. 2A, 2B). Ļ░ÖņØĆ ņÖĖļČĆ ļ│æņøÉņŚÉņä£ ņŗ£Ē¢ēĒĢ£ ņĀäņŗĀ ņ¢æņĀäņ×Éļŗ©ņĖĄņ┤¼ņśü Ļ▓Ćņé¼ņāü ņÜ░ņĖĪ ĒĢśņĢģĻ│©ņŚÉ 18F-fluodeoxy-glucose SUV max 6.8ņØś ņØ┤ņāüņäŁņĘ© ņåīĻ▓¼ ļ░Å ņÜ░ņĖĪ Ļ▓ĮļČĆ ļĀłļ▓© IIņŚÉ ņØ┤ņāüņäŁņĘ© ņåīĻ▓¼ ļ│┤ņśĆļŗż(Fig. 2C). ņØ┤ĒøäņŚÉ ļ│ĖņøÉņŚÉņä£ ņŗ£Ē¢ēĒĢ£ Ļ▓ĮļČĆ ņĀäņé░ĒÖö ļŗ©ņĖĄ ņ┤¼ņśüņāü, ņØ┤ņĀäņØś ļéŁņóģ ņĀüņČ£ņłĀ ļ░Å ļ░£ņ╣ś ņłśņłĀ Ēøä ņÜ░ņĖĪ ĒĢśņĢģĻ│© Ļ│© Ļ▓░ņåÉļČĆņ£ä ļ│┤ņśĆņ£╝ļéś ĻĖłņåŹņ£╝ļĪ£ ņØĖĒĢ┤ ļ│æļ│Ć ļČĆņ£ä ĒÅēĻ░ĆļŖö ņĀ£ĒĢ£ņĀüņØ┤ņŚłĻ│Ā, ņÜ░ņĖĪ Ļ▓ĮļČĆ ļĀłļ▓© IIņŚÉ ņĀäņØ┤Ļ░Ć ņØśņŗ¼ļÉśļŖö ļ”╝ĒöäņĀł ļ╣äļīĆ ņåīĻ▓¼ ļ│┤ņśĆļŗż(Figs. 2D, 2E). ĒĢ┤ļŗ╣ ļ”╝ĒöäņĀłņŚÉ ļīĆĒĢ┤ ņ┤łņØīĒīī ņ£ĀļÅäĒĢś ņäĖņ╣©ĒØĪņØĖĻ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒ¢łņ£╝ļéś, ņäĖĒżļ│æļ”¼Ļ▓░Ļ│╝ņāü ļ░śņØæņä▒ Ļ│╝ĒśĢņä▒ ņåīĻ▓¼ņ£╝ļĪ£ ĒÖĢņØĖļÉśņŚłļŗż.

Fig.┬Ā2
Preoperative images. (A) Axial T1-weighted enhanced MR findings. About 2.3 x 2.0 x 1.2 cm enhancing lesion at right mandible angle with overlying bony cortex erosion (white arrow). (B) Several slightly enlarged lymph nodes without necrosis at right level II (white arrow head). (C) PET-CT findings. Abnormal FDG uptakes in right mandible and right retromolar mucosal space, right level II, III lymph nodes(white arrow head). (D) Contrast enhanced neck CT findings. Postoperative bone defect at right mandible(black arrow). Limited evaluation due to beam hardening artifact. (E) Lymphadenopathy at right level II, r/o Metastatic lymph node(black arrow head).
ņØ┤ņŚÉ ņÜ░ņĖĪ ļČäņĀł ĒĢśņĢģņĀłņĀ£ņłĀ, ļ╣äĻ│©ņØä ņØ┤ņÜ®ĒĢ£ ņ×¼Ļ▒┤ ļ░Å ņÜ░ņĖĪ ņäĀĒāØņĀü Ļ▓ĮļČĆ ņ▓ŁņåīņłĀņØä Ļ│äĒÜŹĒĢśņśĆļŗż. ņłśņłĀ ņĀä ĒĢśņĢģ Ļ▓░ņåÉļČĆņ£ä ĒÖĢņØĖ ļ░Å ņ×¼Ļ▒┤ņØä Ļ│äĒÜŹĒĢśĻĖ░ ņ£äĒĢ┤ 3D printerļź╝ ņØ┤ņÜ®ĒĢśņŚ¼ ĒĢśņĢģ ļ¬©ļŹĖņØä ņĀ£ņ×æĒĢśņśĆļŗż(Fig. 3). ņÜ░ņĖĪ 2ļ▓łņ¦Ė ņ¢┤ĻĖłļŗł ņĢ× ņśüņŚŁļČĆĒä░ ĒĢśņĢģĻ░ü ļ░Å Ļ░Ćņ¦ĆļČĆņ£ä ĒżĒĢ©ĒĢśņŚ¼ ĻĘ╝ļÅīĻĖ░ ņĢäļלļČĆņ£äĻ╣īņ¦Ć ņĀłĻ░£ ļ▓öņ£äļź╝ Ļ│äĒÜŹĒĢśņśĆĻ│Ā, ļ░£ņāØņØ┤ ņśłņāüļÉśļŖö Ļ▓░ņåÉļČĆņ£äņŚÉ ļīĆĒĢśņŚ¼ miniplateļź╝ ļ¦×ņČöņ¢┤ ņżĆļ╣äĒĢśņśĆļŗż. ņłśņłĀņØĆ ņÜ░ņäĀ ĻĖ░Ļ┤ĆņĀłĻ░£ņłĀņØä ņŗ£Ē¢ēĒĢśĻ│Ā ņØ┤ņ¢┤ņä£ ņÜ░ņĖĪ ņäĀĒāØņĀü Ļ▓ĮļČĆ ņ▓ŁņåīņłĀ(Ļ▓ĮļČĆ ļĀłļ▓© I,II,III)ņØä ņŗ£Ē¢ēĒĢśņśĆļŗż. ņé¼ņĀäņŚÉ Ļ│äĒÜŹĒ¢łļŹś ņĀłĻ░£ Ļ▓ĮĻ│äĻ░Ć ļģĖņČ£ļÉĀ ņłś ņ׳ļÅäļĪØ ĒĢśņĢģĻ│©ņØä ņČ®ļČäĒ׳ ļģĖņČ£Ē¢łņ£╝ļ®░, Ļ│äĒÜŹļīĆļĪ£ ļČäņĀł ĒĢśņĢģ ņĀłņĀ£ņłĀņØä ņ¦äĒ¢ēĒĢśņśĆļŗż. ĻĄ¼ņł£ ņĀłĻ░£ņŗ£ ļ░£ņāØĒĢĀ ņłś ņ׳ļŖö ĒØēĒä░ ļō▒ņØä Ļ│ĀļĀżĒ¢łņØä ļĢī, Ēö╝ĒīÉņØä ņ£äļĪ£ ņŚ░ņןĒĢśņŚ¼ ļōżņ¢┤ņś¼ļĀż ņČ®ļČäĒ׳ Ļ▓ĮĻ│äļź╝ ĒÖĢļ│┤ĒĢśļ®░ ņĀłņĀ£ĒĢĀ ņłś ņ׳ņØä Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉśņ¢┤ ĻĄ¼ņł£ ņĀłĻ░£ ņŚåņØ┤ ņ¦äĒ¢ēĒĢśņśĆļŗż. Ļ▓░ņåÉļČĆņ£ä ņ×¼Ļ▒┤ ņ£äĒĢ┤ ņÜ░ņĖĪ ļ╣äĻ│©ņØä ņ▒äņĘ©ĒĢśņśĆņ£╝ļ®░ miniplateļĪ£ Ļ│ĀņĀĢĒĢ£ Ēøä ņłśņłĀņØä ņóģļŻīĒĢśņśĆļŗż(Fig. 4).
Fig.┬Ā3
3D model of the patientŌĆÖs mandible before operation. PatientŌĆÖs CT was analyzed and modeled 3 dimensionally, and the relevant data was transmitted to the Project 360 3D printerŌäó(3D systems, United States). Resection margins were pre-designed for the resection of the mandible from the right second molar area to the inferior part of the coronoid process.

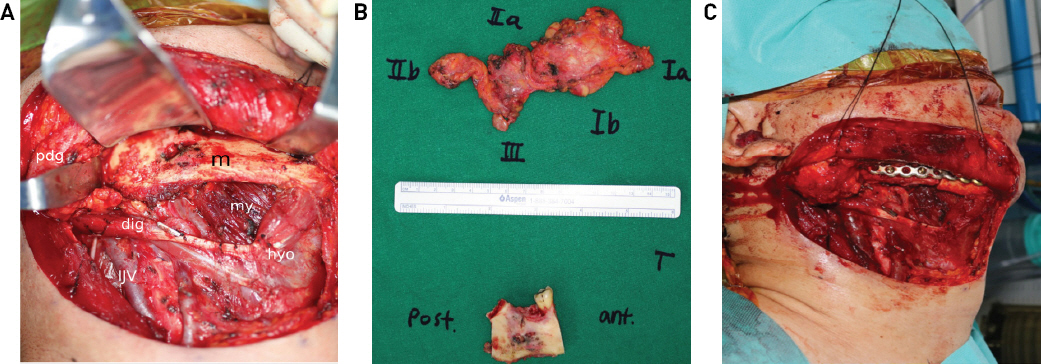
Fig.┬Ā4
Intraoperative photographs. (A) Operative field before segmental mandibulectomy. (B) Surgical specimen. (C) Operative field after segmental mandibulectomy and fibular free flap miniplate fixation. (m : mandible, my : mylohyoid, dig : digastric muscle, hyo : hyoid bone, IJV : internal jugular vein, pdg : parotid gland)
ņĄ£ņóģ ļ│æļ”¼Ļ▓░Ļ│╝ ņāü 2mmņØś ļ│æņåī Ēü¼ĻĖ░ļź╝ Ļ░Ćņ¦ä ĒÄĖĒÅēņäĖĒżņĢö ņåīĻ▓¼ ļ│┤ņśĆņ£╝ļ®░, Ļ▓ĮĻ│äņŚÉ ņĢöņäĖĒżļŖö ņŚåņŚłĻ│Ā, ņ┤Ø 32Ļ░£ņØś ļ”╝ĒöäņĀł ņżæ ņĀäņØ┤ļź╝ ļ│┤ņØ┤ļŖö ļ”╝ĒöäņĀłņØĆ ņŚåņŚłļŗż(Fig. 5). ņłśņłĀ ņ¦üĒøä ĒÖśņ×ÉļŖö ĻĖłņŗØņØä ņ£Āņ¦ĆĒĢśņśĆĻ│Ā, ņłśņłĀ Ēøä 6ņØ╝ņ¦Ė Ļ▓Įļ╣äĻ┤Ć ņŗØņØ┤ ņ¦äĒ¢ēĒĢśņśĆņ£╝ļ®░ ņłśņłĀ Ēøä 14ņØ╝ņ¦Ė Ļ▓ĮĻĄ¼ ņŗØņØ┤ļź╝ ņŗ£ņ×æĒĢśņśĆĻ│Ā ņØ┤Ēøä ĒŖ╣ņØ┤ ĒĢ®ļ│æņ”Ø ņŚåņØ┤ Ēć┤ņøÉĒĢśņśĆļŗż. ņłśņłĀ Ēøä ĒĢ£ ļŗ¼ņ¦Ė ņČöņĀüĻ┤Ćņ░░ ņ£äĒĢ┤ ņŗ£Ē¢ēĒĢ£ ņĢłļ®┤Ļ│© 3D ņĀäņé░ĒÖö ļŗ©ņĖĄ ņ┤¼ņśüņŚÉņä£ Ļ│©Ēö╝ĒīÉ ņĢłņĀĢņĀüņ£╝ļĪ£ ņ£Āņ¦ĆļÉśļŖö Ļ▓āņØä ĒÖĢņØĖĒĢĀ ņłś ņ׳ņŚłļŗż(Figs. 6A, 6B).
Fig.┬Ā5
Pathology of the surgical specimen showing squamous cell carcinoma (SCC) lesion without lymph node metastasis. (A) Gross photo, ill defined brown colored lesion involving mandible. (B) SCC site (H&E staining, x12), ill defined fibrotic lesion with focal viable tumor cells involving trabecular bone. (C) SCC site (H&E staining x100), Tumor cells show round to ovoid nuclei with size variation, occasionally prominent nucleoli, and eosinophilic or clear cytoplasm, consistent with residual carcinoma.
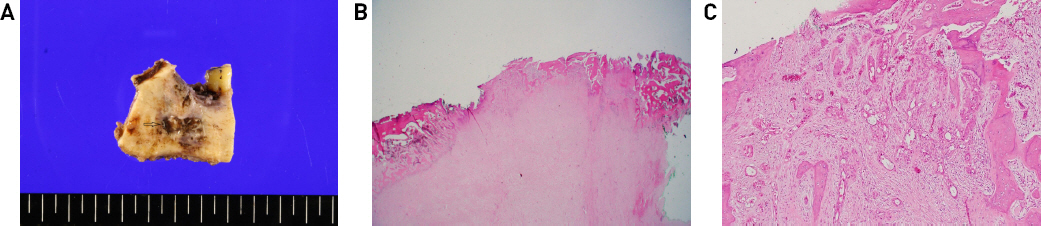
Fig.┬Ā6
Postoperative findings. (A) Facial bone 3D CT findings at 1 month after operation, anterior cut. (B) Lateral cut. (C) Contrast enhanced Neck CT(11 months after operation). No evidence of local tumor recurrence. (D) Intraoral photograph 13 months after operation. (E) Postoperative neck appearance 13 months later.
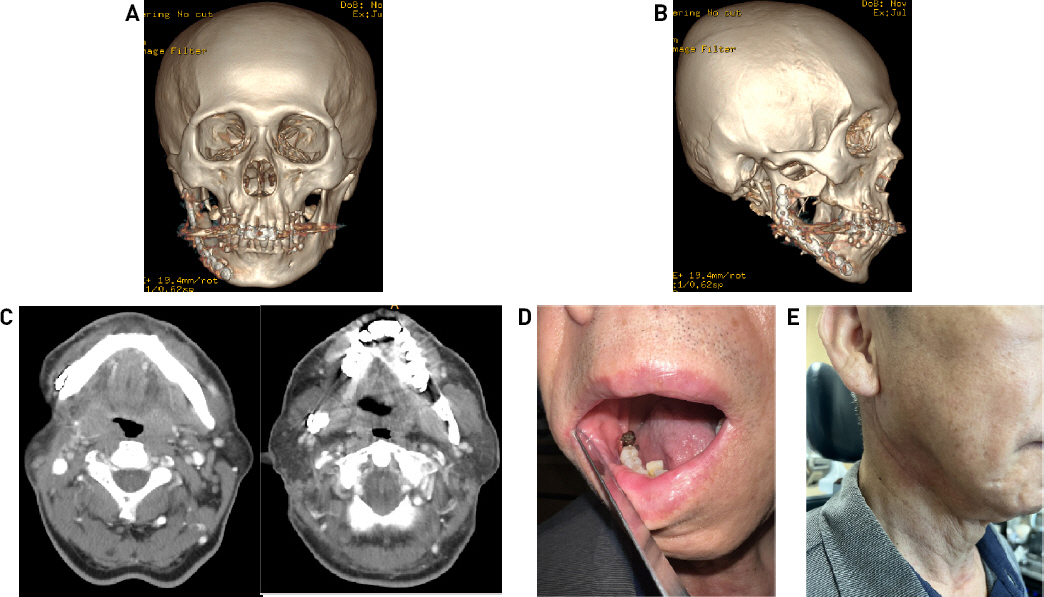
ņłśņłĀ 11Ļ░£ņøö Ēøä ņ┤¼ņśüĒĢ£ Ļ▓ĮļČĆ ņĀäņé░ĒÖö ļŗ©ņĖĄ ņ┤¼ņśü ņāü ņłśņłĀļČĆņ£ä ĒŖ╣ņØ┤ ņØ┤ņāü ņåīĻ▓¼ņØ┤ļéś ņ×¼ļ░£ ņåīĻ▓¼ ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśņ£╝ļ®░(Fig. 6C), ĒÖśņ×ÉļŖö ņłśņłĀ Ēøä 13Ļ░£ņøöĻ╣īņ¦Ć Ļ▓ĮļČĆ ļ░Å ĻĄ¼Ļ░Ģ ļé┤ ņłśņłĀļČĆņ£ä ĒŖ╣ņØ┤ņé¼ĒĢŁ ļ│┤ņØ┤ņ¦Ć ņĢŖņ£╝ļ®░ ļö▒ļö▒ĒĢ£ ņØīņŗØņØä ņĀ£ņÖĖĒĢ£ ņØ╝ļ░ś ņŗØņØ┤Ļ░Ć ņ¦äĒ¢ē Ļ░ĆļŖźĒĢ£ ņāüĒā£ļĪ£ ņČöņĀü Ļ┤Ćņ░░ ņżæņØ┤ļŗż(Figs. 6D, 6E).
Ļ│Āņ░░
ņĢģĻ│©ņŚÉ ļ░£ņāØĒĢśļŖö ņĢöņóģņØĆ ņāüļīĆņĀüņ£╝ļĪ£ ļō£ļ¼╝ļ®░, ļŗżņ¢æĒĢ£ ņĪ░ņ¦üĒĢÖņĀü ņåīĻ▓¼Ļ│╝ ņØ┤ņŚÉ ļö░ļźĖ ļŗżņ¢æĒĢ£ ņ×äņāü ņ”Øņāü ļ░Å ņśłĒøäļź╝ ļ│┤ņØĖļŗż. ņĪ░ņ¦üĒĢÖņĀü ņåīĻ▓¼ņŚÉ ļö░ļØ╝ 1) ĒāĆņĢĪņäĀ ņĢöņóģ, 2) ņ╣śņä▒ ņĢöņóģ, 3) ņ╣śņä▒ ļéŁņóģņŚÉņä£ ĻĖ░ņøÉĒĢ£ ņøÉļ░£ņä▒ Ļ│©ļé┤ ĒÄĖĒÅēņāüĒö╝ņäĖĒż ņĢöņóģņ£╝ļĪ£ ļČäļźśĒĢĀ ņłś ņ׳ļŗż.4) ņØ┤ ņżæ PIOSCCļŖö 1913ļģä LoosņŚÉ ņØśĒĢ┤ ņ▓śņØī ļ│┤Ļ│ĀļÉśņŚłņ£╝ļ®░, ņ╣śņä▒ ļéŁņóģņŚÉņä£ ĻĖ░ņøÉĒĢśļŖö ņøÉļ░£ņä▒ Ļ│©ļé┤ ĒÄĖĒÅēņäĖĒżņĢöņ£╝ļĪ£, ļ░£ņāØļźĀņØĆ 0.31-3%ļĪ£ ņČöņĀĢļÉśļéś, PIOSCCņØś ņ¦äļŗ©ĻĖ░ņżĆņØ┤ ļ│ĆĒĢśĻ│Ā ņĪ░ņ¦üĒĢÖņĀü ļČłĒÖĢņŗżņä▒ņØ┤ ņ׳ņ¢┤ ņĀĢĒÖĢĒĢ£ ņ£Āļ│æļźĀņØä ņĢī ņłś ņŚåļŖö ņŗżņĀĢņØ┤ļŗż.3,5)
PIOSCCļŖö Ēü¼Ļ▓ī ņ╣śņä▒ ļéŁņóģ ĻĖ░ņøÉĻ│╝ ņ╣śņä▒ Ļ░üĒÖöļéŁ ĻĖ░ņøÉņ£╝ļĪ£ ĻĄ¼ļ│äĒĢĀ ņłś ņ׳ņ£╝ļ®░, Ēøäņ×ÉĻ░Ć ņĀäņ×ÉņŚÉ ļ╣äĒĢ┤ ļō£ļ¼╝ļŗż. ņ×äņāüņĀü, ņśüņāüĒĢÖņĀü ņåīĻ▓¼ņ£╝ļĪ£ļŖö ļæÉ ņ¦äļŗ© ņé¼ņØ┤ņŚÉ Ēü░ ņ░©ņØ┤Ļ░Ć ņŚåņ£╝ļéś ņ╣śņä▒ Ļ░üĒÖöņä▒ ļéŁņóģņØĆ ļŗżļźĖ ņ╣śņä▒ ļéŁņóģļōżĻ│╝ ļ╣äĻĄÉĒ¢łņØä ļĢī, ĒŖ╣ņØ┤ĒĢ£ ņĪ░ņ¦üĒĢÖņĀü ĒśĢĒā£ļź╝ ļéśĒāĆļéĖļŗż.6) ņŻ╝ļĪ£ 6-8ņĖĄņØś ņ¢ćņØĆ ņżæņ”ØĻ░üĒÖöĒÄĖĒÅēņāüĒö╝(stratified keratinizing squamous epithelium)ļĪ£ ņØ┤ļŻ©ņ¢┤ņĀĖ ņ׳ņ£╝ļ®░, ļīĆļČĆļČäņØĆ ņ░®Ļ░üĒÖöņĖĄņØ┤ļéś ļĢīļĪ£ļŖö ņ¦äņä▒Ļ░üĒÖöņĖĄņØ┤ļ®░, ņä¼ņ£Āņä▒ ļéŁņóģ ļ▓ĮņØ┤ ņ¢ćņ£╝ļ®░ ņŚ╝ņ”ØņäĖĒżĻ░Ć ņĀüļŗż. ļŗ©ļ░▒ņ¦łņØ┤ 3.5ml/dLļ│┤ļŗż ņĀüņØĆ ļ¦æņØĆ ļ¼╝ ņä▒ļČäņŚÉņä£ ņ╝ĆļØ╝Ēŗ┤ņ£╝ļĪ£ ņ▒äņøīņ¦ä ņä▒ļČäĻ╣īņ¦Ć ļŗżņ¢æĒĢśļ®░, ļ▓ĮņŚÉ ļöĖļéŁ(daughter cyst) ņØ┤ ņĪ┤ņ×¼ĒĢśļŖö ĒŖ╣ņ¦ĢņØ┤ ņ׳ļŗż.2) ņØ┤ ņżæ, ĒĢśļéś Ēś╣ņØĆ ĻĘĖ ņØ┤ņāüņØś ļöĖļéŁĻ│╝ ņāüĒö╝ ĻĖ░ņĀĆņĖĄņØś ļ░£ņĢä(budding)Ļ│╝ Ļ░ÖņØĆ ņ╣śņä▒ Ļ░üĒÖöņä▒ ļéŁņóģņØś ņĪ░ņ¦üĒĢÖņĀü ĒŖ╣ņ¦ĢņØĆ ļåÆņØĆ ņ×¼ļ░£ļźĀĻ│╝ Ļ┤ĆļĀ©ņØ┤ ņ׳ļŗżĻ│Ā ļ│┤Ļ│ĀļÉśĻ│Ā ņ׳ļŗż.7) ņ╣śņä▒ Ļ░üĒÖöņä▒ ļéŁņóģņØś ņ×¼ļ░£ļźĀņØĆ 5ļģäĻ░ä 0-62%ņØś ļŗżņåī ļäōņØĆ ļ▓öņ£äļĪ£ ļ│┤Ļ│ĀļÉśļ®░, ņØ┤ļŖö ņŚ░ĻĄ¼ ļööņ×ÉņØĖĻ│╝ ĒåĄĻ│äĒĢÖņĀü ļ░®ļ▓ĢņØ┤ ļŗżļźĖ ņØ┤ņ£Āļ┐Éļ¦ī ņĢäļŗłļØ╝, ļ│æļ│Ć ņ×Éņ▓┤ņØś ļ░£ņāØļźĀņØ┤ ļé«ņØĆļŹ░ ĻĖ░ņØĖĒĢ£ļŗż.8)
ņ╣śņä▒ Ļ░üĒÖöņä▒ ļéŁņóģņØś ņĢģņä▒ ļ░£Ēśä ĻĖ░ņĀäņØĆ ļ¬ģĒÖĢĒĢśĻ▓ī ļ░ØĒśĆņ¦Ćņ¦Ć ņĢŖņĢśņ¦Ćļ¦ī, Van der wal9) ļō▒ņØĆ ļéŁņóģņØś Ļ░üņ¦łĒÖöĻ░Ć ņĢģņä▒ ļ│ĆĒÖś Ļ░ĆļŖźņä▒ņØä ļåÆņØĖļŗż ĒĢśļ®░, Gardner,10) Yu11) ļō▒ņØĆ ņśżļל ņ¦ĆņåŹļÉ£ ļ¦īņä▒ ņŚ╝ņ”ØņØ┤ ņĢģņä▒ ļ│ĆĒÖöņØś ņäĀĒ¢ē ņÜöņØĖņØ┤ļØ╝ ļ│┤Ļ│ĀĒĢ£ ļ░ö ņ׳ļŗż. ņŻ╝ ĻĖ░ņĀäņØĆ ļ¦īņä▒ ņŚ╝ņ”ØņØ┤ ņśżļל ņ¦ĆņåŹļÉśļ®┤ņä£ ĒÖ£ņä▒ņé░ņåī ļīĆņé¼ļ¼╝ņØä ĒśĢņä▒ĒĢśļ®░, DNA, ļŗ©ļ░▒ņ¦ł, ņäĖĒżļ¦ēņŚÉ ņåÉņāüņØä ņŻ╝Ļ│Ā ņĀĢņāü ņäĖĒżņé¼ļ®Ė(apoptosis)ņÖĆ ļ░śļīĆļĪ£ ņóģņ¢æņäĖĒżņØś ļ│┤ņāüņĀü ņ”ØņŗØļ░śņØæņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż.12)
ņ╣śņä▒ Ļ░üĒÖöņä▒ ļéŁņóģņØĆ ņĢģĻ│©ņØś ļéŁ ņżæņŚÉņä£ 3-11% ņĀĢļÅäļź╝ ņ░©ņ¦ĆĒĢśļ®░, Ēü¼ĻĖ░Ļ░Ć Ēü¼ļŹöļØ╝ļÅä ņ┤łĻĖ░ņŚÉļŖö ļ¬ģĒÖĢĒĢ£ ņ”ØņāüņØ┤ ņŚåļŗż. ļĢīļĢīļĪ£, ĒÖśņ×ÉļōżņØĆ ļČĆņóģ, ĒåĄņ”Ø, ņØ┤ņāüĻ░ÉĻ░ü, ņ╣śņĢä ĒØöļōżļ”╝ ļō▒ņØś ņ”ØņāüņØä ĒśĖņåīĒĢśļ®░ ņØ┤ ņżæ Ļ░Ćņן ĒØöĒĢ£ Ļ▓āņØĆ ļČĆņóģņØ┤ļŗż.13,14) ņØ┤ļōżņØĆ ļåÆņØĆ ņ×¼ļ░£ņ£©ņØä ļ│┤ņØ┤Ļ│Ā, Ļ│ĄĻ▓®ņĀüņØĖ ņä▒Ē¢źņØä ļØĀĻĖ░ ļĢīļ¼ĖņŚÉ ņ×äņāüņĀüņ£╝ļĪ£ ņŻ╝ņØśĻ░Ć ņÜöļ¦ØļÉśļŖö ļéŁņóģņØ┤ļŗż. ļŗżņØīņØĆ ĻĖ░ņĪ┤ņŚÉ ļ│┤Ļ│ĀļÉ£ ņ╣śņä▒ Ļ░üĒÖöņä▒ ļéŁņóģņŚÉņä£ ļ░£ĒśäļÉ£ ĒÄĖĒÅēņäĖĒżņĢöņóģņŚÉ ļīĆĒĢ£ ņ”ØļĪĆļź╝ ņĀĢļ”¼ĒĢ£ Ēæ£ņØ┤ļŗż(Table 1).
Table┬Ā1
Reported cases of squamous cell carcinoma arising from an OKC
ņĀĆņ×ÉļōżņØĆ ņØ┤ļ▓ł ņ”ØļĪĆļź╝ ĒåĄĒĢśņŚ¼ ļīĆļČĆļČäņØś ņ╣śņä▒ Ļ░üĒÖöņä▒ ļéŁņóģņØĆ ņ¢æņä▒ņØ┤ļéś, ļō£ļ¼╝Ļ▓ī ņĢģņä▒ Ļ░ĆļŖźņä▒ņØ┤ ņ׳ĻĖ░ ļĢīļ¼ĖņŚÉ, ļ¬©ļōĀ ņ╣śņä▒ Ļ░üĒÖöņä▒ ļéŁņóģņŚÉ ļīĆĒĢ£ ņäĖņŗ¼ĒĢ£ Ēśäļ»ĖĻ▓ĮņĀü Ļ┤Ćņ░░ņØ┤ ĒĢäņÜöĒĢśļŗżļŖö Ļ▓āņØä Ļ▓ĮĒŚśĒĢśņśĆļŗż. ļśÉĒĢ£, ņ╣śņä▒ Ļ░üĒÖöņä▒ ļéŁņóģņŚÉņä£ ņĪ░ļīĆņłĀ ļ░Å ņĀüņČ£ņłĀņØä ņŗ£Ē¢ēĒĢĀ ņŗ£, ņ×öņŚ¼ ņāüĒö╝ ļ░Å ļéŁļ▓ĮņØś ļöĖļéŁņØś ņĪ┤ņ×¼ļĪ£ ņ×¼ļ░£ ļ░Å ņĢģņä▒ ņĀäĒÖś Ļ░ĆļŖźņä▒ņØ┤ ņ׳ĻĖ░ ļĢīļ¼ĖņŚÉ ņŻ╝ņØśĻ░Ć ĒĢäņÜöĒĢśļŗż.15) ļö░ļØ╝ņä£ ņ×¼ļ░£ņØ┤ ļ░śļ│ĄļÉĀņłśļĪØ ņŚ╝ņ”ØņØä ņĢģĒÖöņŗ£Ēé¼ ļ┐Éļ¦ī ņĢäļŗłļØ╝, ņāüĒö╝ņäĖĒżņØś ņĢģņä▒ ņĀäĒÖś Ļ░ĆļŖźņä▒ ļśÉĒĢ£ ņ”ØĻ░ĆļÉśļ»ĆļĪ£, ņ”ØņāüņØ┤ ņśżļלļÉśĻ▒░ļéś ņ×¼ļ░£ņØ┤ ņ×”ņØä Ļ▓ĮņÜ░ ĒÄĖĒÅēņäĖĒżņĢöĻ│╝ ļÅÖļ░śļÉśņŚłņØä Ļ░ĆļŖźņä▒ņØä ņŚ╝ļæÉņŚÉ ļæÉĻ│Ā ņäĖņŗ¼ĒĢ£ ĒÅēĻ░ĆĻ░Ć ĒĢäņÜöĒĢĀ Ļ▓āņØ┤ļŗż.




