

Introduction
EwingŌĆÖs sarcoma, a small round cell tumor, arises from primitive mesenchymal stem cells found in the bone marrow. Typically, this tumor is distinguished by the presence of a fusion transcript involving EWS-FLI1 or EWS- ERG. The lower extremities and pelvis of adolescents are common sites of skeletal origin, and the trunk is the most common extra-skeletal site.1) It is extremely rare for EwingŌĆÖs sarcoma to have its primary site in the larynx. To date, only few such cases have been reported.2)
Laryngeal cancer accounts for less than 1% of all cancers, and among them, squamous cell carcinoma accounts for more than 95%.2,3) Laryngeal sarcoma is very rare, accounting for less than 1% of laryngeal cancers, and among its subtypes, chondrosarcoma is much more common than other types.2) As the treatment approach for cancer can vary depending on the stage, complete mass excision through laryngeal microsurgery (LMS) or radiation therapy is a common treatment option for early stage cancer.3,4) The main symptoms in patients with vocal cord lesions are hoarseness or vocal fatigue, and occasionally experience difficulty in breathing. Typically, excisional biopsy vis LMS is used for both diagnosis and treatment.5)
We report a case in which a vocal fold polyp was suspected preoperatively and diagnosed as an extraskeletal EwingŌĆÖs sarcoma (EES) after surgical resection.
Case report
A 17-year-old man presented to the Department of Otorhinolaryngology with complaints of voice change for a month. The patient did not have any underlying comorbidities and did not present with any other symptoms. The patient was a high school student with no history of voice abuse or misuse, and denied any smoking history.
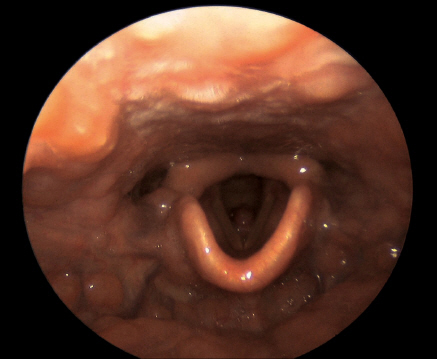
Laryngoscopy revealed a mass-like lesion in the left vocal folds. A pinkish round mass approximately 1 cm in size was observed anterior to the left vocal fold, which was suspected to be a polyp based on clinical evaluation (Fig. 1). Based on the size of the mass, surgical removal was deemed necessary, and LMS was planned.
Fig.┬Ā1
Preoperative laryngoscope. A round, pinkish mass, approximately 1 cm in size, was observed anterior to the left vocal fold.
Stroboscopy examination and computed tomography (CT) scanning were not performed before surgery.
In the surgical field, we found a soft mass in the left vocal fold, which was located at the level of the epithelium and demarcated from the surroundings. The mass was dissected from the vocal-fold epithelium using a cold instrument. Because malignancy was not suspected during surgery, the mass was dissected without a safety margin. There were no specific findings in the larynx or hypopharynx except for a vocal fold mass. Following surgery, no residual mass was observed and there were no complications such as bleeding or respiratory distress (Fig. 2).
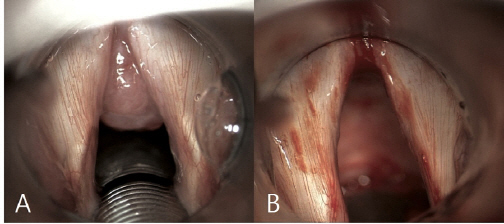
Fig.┬Ā2
Laryngeal microsurgery intraoperative microscope image. The mass previously noted on laryngoscopy was attached to the left anterior vocal cord (A), and there was no gross residual tumor after cold knife dissection (B).
On histopathological examination, the tumor was 1.2 x 0.9 cm in sisze, and hematoxylin and eosin staining revealed that the tumor was composed of spindle cells. The resection margin of the tumor was indeterminate in pathologic report. The cells stained positive for CD99 and BCL2 and were focally positive for TLE1 (Fig. 3).
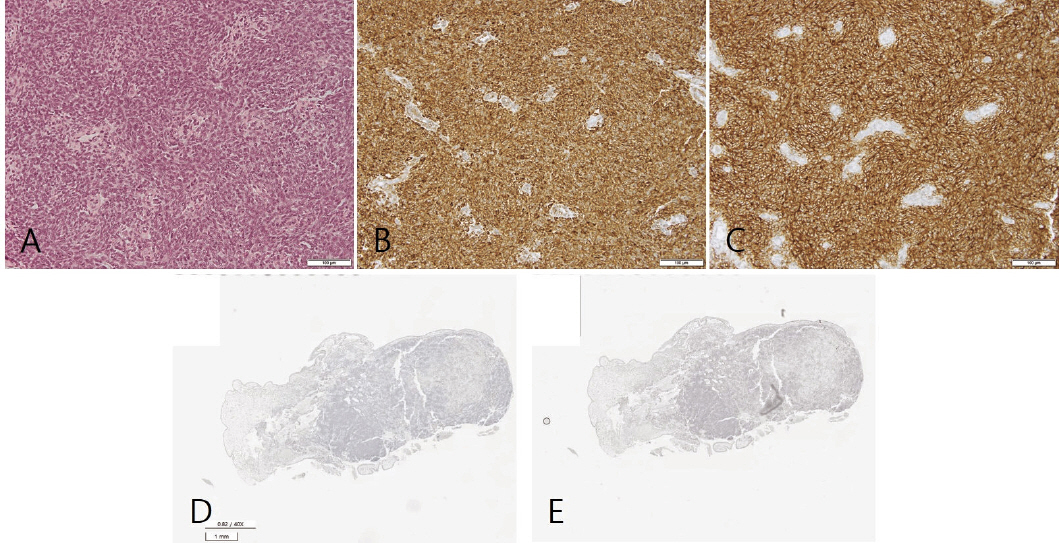
Fig.┬Ā3
Microscopic findings. The tumor was composed of oval-to-spindle cells with scant clear-to-eosinophilic cytoplasm and showed a wheel-like growth pattern. Cytoplasmic membranes were indistinct (A, x100, H&E). The tumor cells were positive for Bcl-2 (B, x100) and showed strong diffuse membranous expression of CD99 (C, x100) on immunohistochemical staining. TLE-1 (D) and SS18-SSX (E) were focally positive in the tumor (x40).
Since the tumor was composed of spindle cells that stained positive for CD99 and BCL2 and weakly positive for TLE1 on IHC, we primarily diagnosed it as a synovial sarcoma. However, ultimately TLE1 was interpreted as negative, and an additional test performed on SS18-SSX was negative (Fig. 3). Therefore, we proceeded with next-generation sequencing (NGS) to confirm the presence of the EWSR1-ERG fusion gene, which indicated EwingŌĆÖs sarcoma.
Postoperative CT scanning and positron emission tomography (PET) were performed and revealed no evidence of locoregional or distant metastases. Adjuvant therapy was necessary after multidisciplinary consultation. The patient underwent chemotherapy (vincristine, doxorubicin, and cyclophosphamide alternating with ifosfamide and etoposide), followed by radiation therapy. The patient has been under 2-year follow-up after treatment, during which there was no evidence of recurrence based on medical history, physical examinations, and imaging studies.
Discussion
Extraskeletal EwingŌĆÖs sarcoma primarily arising from the head and neck region accounts for approximately 4-9% of all cases, with a predominant report of cases in the nasal cavity, oral cavity, sinuses, or soft tissue of the neck.6) Less than 10 cases have been reported to date (Table 1).7) These cases showed a generally irregular shape and a pattern of spreading to surrounding tissues.2,8,9)
Table┬Ā1
Summary of published articles on laryngeal wing sarcomas
To diagnose EwingŌĆÖs sarcoma, it is important to perform a biopsy after clinical suspicion. Histologically, Ewing is characterized by small cells with round nuclei. CD99 is highly sensitive, but has very low specificity. Synovial sarcoma, rhabdomyosarcoma, and chondrosarcoma are also CD99 positive. Therefore, FLI1, which has a higher specificity, is important. Currently, molecular pathology is essential for diagnosing EwingŌĆÖs sarcoma, which lacks characteristic features. FISH-based detection of EWSR1 has been used for decades since the introduction of NGS technology, and it has become possible to diagnose EwingŌĆÖs sarcoma by detecting fusion genes, such as EWSR1-ERG.10)
EwingŌĆÖs sarcoma of the head and neck is rare; thus, treatment plans are based on cases involving more common sites, such as the lower extremities or pelvis.11) In the case of skeletal EwingŌĆÖs sarcoma, standard treatment involves multiagent induction chemotherapy followed by local treatment with surgery, definitive radiation, or a combination of surgery and radiation followed by additional chemotherapy and consolidation of local treatment to metastatic sites.1) It has been reported that the treatment outcomes of head and neck EwingŌĆÖs sarcoma and skeletal EwingŌĆÖs sarcoma are similar.11)
In our case, the initial impression was a benign vocal fold lesion based on the preoperative laryngoscopy findings; therefore, imaging work-up was not considered prior to surgery, and incidentally, EES was diagnosed after the LMS biopsy. Resection margins were not secured, and adjuvant therapy was administered based on postoperative evaluation and multidisciplinary discussions.
Laryngeal EwingŌĆÖs sarcoma is a rare cancer, and its diagnosis has been challenging owing to the atypical presentation of reported cases. The current standard treatment of EwingŌĆÖs sarcoma is neoadjuvant and adjuvant chemotherapies in conjunction with surgery and/or radiotherapy to manage the primary site and potential metastatic disease. During surgery, efforts are made to achieve a resection margin, if feasible.1) In our case, due to the lack of clear margin definition, adjuvant concurrent chemoradiotherapy was administered. As of a 2-year follow-up, the patient remains under surveillance with no evidence of recurrence. We aimed to present this rare case to contribute to the diagnosis and treatment of EwingŌĆÖs sarcoma in the future, with the hope of providing valuable insights and clinical evidence.




