부갑상선 선종으로 인한 자발적 경부 혈종 1예
A Case of Spontaneous Cervical Hematoma caused by Parathyroid Adenoma
Article information
Abstract
= Abstract =
Spontaneous cervical hematomas could lead to life-threatening complications, and aneurysms, retopharyngeal abscesses, parathyroid adenomas, laryngeal cysts, and neurogenic tumors should be distinguished as possible underlying causes. Symptoms accompanying spontaneous cervical hematoma include cervical swelling, ecchymosis, dysphagia, dyspnea and hoarseness. We recently experienced a case of spontaneous cervical hematoma in a 52-year-old woman, who initially presented with cervical swelling after severe coughing two days ago. Resultingly parathyroid adenoma was finally confirmed after mass excision. Therefore, we present this unique case with a review of the literature.
서론
부갑상선 종양은 약 85%의 부갑상선 선종과 약 15%의 부갑상선 증식증, 약 1% 이하의 부갑상선 암종으로 구성된다.1) 부갑상선 선종은 낭성 종물로 드물게 피막 외 자연 출혈을 일으켜 갑작스런 경부 종창과 피하 반상 출혈(ecchymosis), 음성 변화, 호흡곤란, 연하 곤란 등을 초래할 수 있으며, 종격동까지 파급될 경우 대동맥 박리로 오인될 수도 있다.2)
최근 저자들은 전경부의 피하 반상 출혈을 동반하여 내원한 부갑상선 선종의 피막외 출혈을 1예 경험하였기에, 문헌고찰과 함께 보고하는 바이다.
증례
52세 여자 환자가 2일 전 심하게 기침을 한 뒤부터 시작된 전경부 통증과 종창 주소로 본원 응급실에 내원하였다. 특이 수술력, 약물 복용력 및 외상력 등의 과거력은 없었으며, 호흡곤란과 음성의 변화는 호소하지 않았다. 이학적 검사상에서 활력 징후는 정상 범위였고, 전경부 부위의 전반에 걸쳐 피하 반상 출혈(ecchymosis)이 관찰되었으며 촉진시에 통증을 호소하였다(Fig. 1A). 후두 내시경 검사상 성대의 움직임은 정상이었고, 후두 점막 전반에 광범위한 반상 출혈(ecchymosis)이 관찰되었다(Fig. 1B).
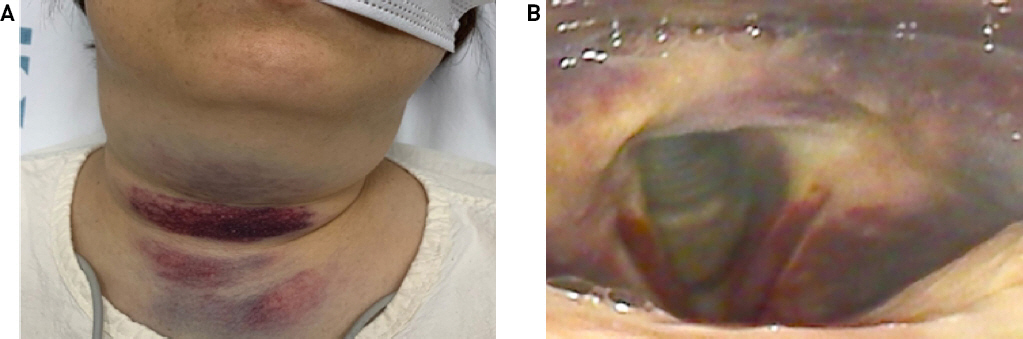
Initial presentation of the patient. A) Gross photograph showing diffuse subcutaneous ecchymosis of anterior neck. B) Laryngoscopic image showing diffuse submucosal ecchymosis of laryngeal mucosa
경부 전산화 단층 촬영 검사에서 갑상선 근처 기관의 좌측 후방에 위치한 3.5cm 크기의 타원형의 종물이 보였고, 종물 내부에 활동성 출혈이 동반된 소견이 보였다(Fig. 2). 경부 출혈에 대한 처치로 경부 탐색술을 고려하였으나 광범위한 혈종으로 인해 탐색술 중 반회후두신경과 식도 손상 가능성을 고려하여, 신경외과 협의 진료 하 혈관조영술을 시행하여 좌측 상갑상선동맥으로부터 혈류를 공급받는 종양을 확인하고 코일 색전술을 시행하였다(Fig. 3). 코일 색전술 후 3일째 시행한 경부 자기공명 영상 촬영 검사 상에서 더 이상 활동성 출혈은 없었고, 종물은 신경원성 종양이 의심되었다(Fig. 4). 향후 혈종이 줄어든 후에 경부 종양 제거술을 계획하고 코일 색전술 후 5일째 이상소견 없이 퇴원하였다. 코일 색전술 후 13일째 기억력 감퇴 및 실어증을 호소하여 촬영한 뇌 전산화 단층 촬영 검사 및 뇌 자기공명 영상 촬영 검사에서 좌측 전두엽 및 전두엽의 아급성 뇌경색이 확인되어 본원 신경외과에서 보존적 치료하며 경부 종양 제거술 시기를 조정하였다.

Axial images of initial CT scan showing a 3.5 cm sized, ovoid mass-like lesion. (A) with active internal bleeding (B, arrow) located at left posterolateral to trachea and esophagus.

Angiographic findings. (A) Feeding vessel to the tumorous lesion was noted originating from the left superior thyroid artery. (B) Artery coiling and embolization was performed.
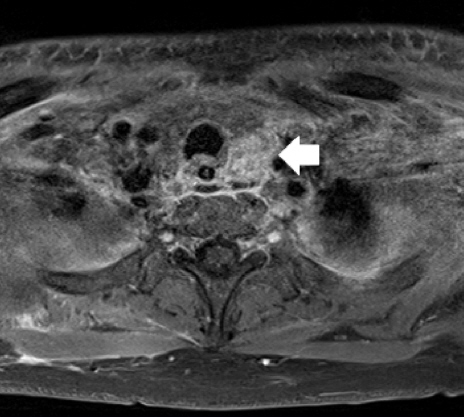
Post-embolization gadolinium-enhanced axial T1-weighted MRI showing a prevertebral mass of 3.5cm size in left posterolateral aspect of trachea and esophagus (white arrow).
코일 색전술 후 90일째, 환자 신경학적 증상 호전되어, 경부 종양 제거술을 시행하기 위해 시행한 경부 전산화 촬영검사와 경부 자기공명 영상 촬영검사 상에서 이전에 보이던 경부 출혈 및 혈종은 모두 흡수된 상태에서 좌측 갑상선 하방의 2.3 cm 크기의 비균질성으로 조영 증강 되는 종물이 확인되었고, 수술 전 부갑상선호르몬(Parathyroid hormone, PTH) 135.41 pg/dL, 혈청 칼슘 11.1 mg/dL, 인 2.7 mg/dL 확인되어 부갑상선선종이 의심되었다(Fig. 5). 수술 중에 좌측 하부 부갑상선이 3cm 크기의 달걀 모양으로 커져 있었고, 주변 혈관들이 많이 발달된 양상이 보였으며, 반회후두신경을 보존한 채로 부갑상선선종을 완전히 제거하였다(Fig. 6). 수술 이후 양측 성대 움직임은 이상 없었으며, 수술 직전 부갑상선호르몬은 535 pg/dL 에서 수술 직후 46 pg/dL 로 감소하였고, 수술 전 혈청 칼슘은 10.7 mg/dL 에서 수술 후 10.2 mg/dL로 감소하였다.
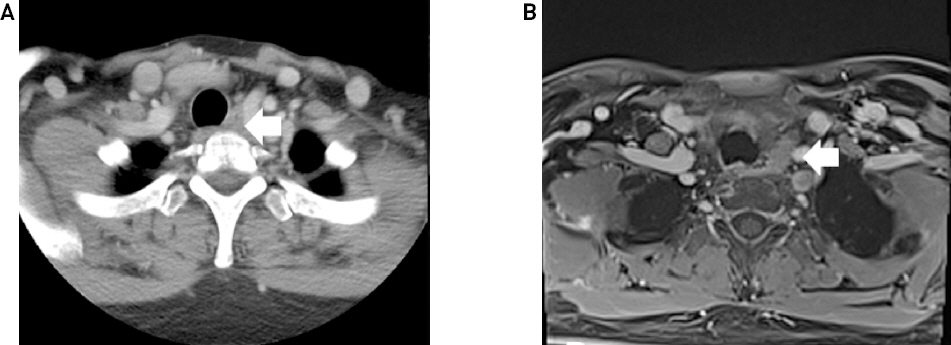
Preoperative CT scan(A, white arrow) and T1-weighted MRI(B, white arrow) showing a 2.3cm sized heterogenous enhancing mass located inferior to the thyroid gland.

Operative photographs. (A) Intraoperative surgical field showing parathyroid adenoma (white arrow) and left thyroid gland(asterix). (B) Gross photograph of the resected surgical specimen.
수술 후 2일째 혈청 칼슘 9.1 mg/dL로, 사지의 저린감이나 입 주위의 이상감각 호소는 없었고, 연축성 경련 등의 증상 호소 없이 퇴원하였다. 적출된 종물의 조직병리 소견상 최종적으로 부갑상선 선종이 확인되었다. 수술 후 3개월 째 시행한 경부 전산화 촬영 검사에서 부갑상선 선종의 재발이나 기타 특이 소견 보이지 않았으며, 수술 후 7개월째 부갑상선호르몬은 43.30 pg/dL, 혈청 칼슘 10.0 mg/dL 로 정상 범위 내로 확인되어 추적 관찰 중이다.
고찰
경부의 반상 출혈과 자연적인 종창은 생명을 위협하는 합병증의 징후일 가능성이 있으며, 발생 가능한 원인으로 동맥류, 후인두 농양, 부갑상선 선종, 후두 낭종, 신경원성 종양 등을 감별해야 한다.3-6)
경부 혈종이 생겼을 때 동반되는 증상으로는 경부 종창, 반상 출혈, 기관과 식도가 압박되어 발생하는 연하 곤란과 호흡곤란, 애성이 있다.7) Simcic 등8)은 부갑상선 선종의 출혈에 의한 경부 혈종은 경부 종창과 피하 반상 출혈, 고칼슘혈증을 보인다고 보고한 바 있다. 본 증례에서는 환자가 응급실에 처음 내원시에 경부 종창과 피하 반상 출혈을 호소하였다. 응급실에서 시행한 경부 전산화 단층촬영 검사 상에서 기관 좌측 후방으로의 종물이 보였으나 주변의 광범위한 혈종으로 인해 영상학적 검사에서 종양의 종류를 특정하기 어려웠으나, 응급실 내원 당시의 혈청 칼슘 수치는 10.1 mg/dL 이었으며, 코일 색전술 후 3일째 혈청 칼슘 수치는 11.8 mg/dL 로 조금 상승하는 소견이 있었다. 본 증례와 같이 경부 혈종을 주소로 내원한 환자에서 경부 종물이 있을 경우, 혈청 칼슘 수치의 상승 여부를 참고한다면 부갑상선 종양의 출혈에 의한 혈종 여부를 감별하는데 도움이 될 것으로 생각된다. 본 증례에서는 수술적 경부 탐색술을 통한 지혈술을 시행할 경우, 주변의 광범위한 혈종과 더불어 종양의 기원이 무엇인지 명확하게 규명하지 못하고 수술 진행 중 반회후두신경이나 식도 손상 등의 합병증 가능성이 높다고 판단되었기에 우선적으로 코일 색전술을 통한 지혈술을 시행하였고, 경부 혈종이 충분히 줄어든 다음 경부 종물에 대한 검사를 재시행하여 수술적 제거를 계획하였다. 경부 종물에서 발생한 급성 출혈 환자에 있어서 수술적 경부 탐색술과 더불어 혈관내 색전술 또한 치료의 선택지로서 충분히 고려할 수 있을 것이다. Ireneusz 등9)은 진행된 두경부 암종에서 급성 출혈의 수술 전 처치 또는 고식적 치료로서 혈관 내 색전술이 효과적임을 발표하였다.
부갑상선 선종의 자연 출혈시에 발생할 수 있는 합병증으로 드물지만 성대 마비가 보고된 바 있다.10,11) 자연 출혈에 의한 성대 마비가 발생하는 기전은 명확하게 밝혀 지지는 않았다. 본 증례의 경우에 후두 내시경상에서 후두 점막 전반에 걸친 반상 출혈은 있었으나 성대 마비는 보이지 않았다. 그러나 경부 부종이 있는 환자에서 성대 마비가 동반될 경우 호흡곤란이 급격히 악화될 수 있으므로 세심하게 확인해야 할 것으로 생각한다.
저자들은 본 증례를 통해 경부 종물과 함께 동반된 경부 급성 출혈 환자가 내원할 경우, 부갑상선 선종에서의 출혈의 가능성을 의심해 보며, 혈중 칼슘 수치와 부갑상선호르몬이 상승되어 있는지 검사가 필요함을 경험하였다. 또한 경부 혈종과 함께 성대 마비나 혈종에 의한 상기도 폐쇄가 발생할 수 있기 때문에 반드시 성대의 움직임을 확인하고 호흡 곤란 등의 증상이 발생하지는 않는지 확인해야 하며, 상기도 폐쇄 발생시 기도 확보가 필요함을 경험하였기에 문헌 고찰과 함께 보고하는 바이다.