상순 구순점막에 발생한 점액낭선암종 1예
A Case of Mucinous Cystadenocarcinoma in Labial Mucosa of Upper Lip
Article information
Abstract
= Abstract =
Mucinous cystadenocarcinoma (MCA) is a malignant tumor that mainly occurs in the breast or ovary, but MCA is internationally rarely reported in head and neck region. Especially MCA in minor salivary gland of oral cavity is even more rare. It is characterized by cystic spaces lining of epithelial cells containing intracytoplasmic mucin. We report a case of MCA in the labial mucosa of upper lip considered to develop from minor salivary gland with a review of literatures.
서론
점액낭선암종은 샘상피조직에서 분화된 비정상적 점액 분비능을 특징으로 하는 악성 암종이다. 1) 입술에서 발생하는 침샘 선암, 그 중에서도 점액낭선암종은 매우 드물다. 2) 점액낭선암종은 조직학적으로 점액을 생성하는 낭성(cystic) 조직을 가진 것을 특징으로 하는 암종으로 유두 성분(papillary component)는 존재하거나 존재하지 않을 수도 있다. 3) 점액낭선암종은 샘상피 기관(glandular organ)이 있는 곳에서 발생 가능하며, 유방, 난소, 췌장 등에서 보고되었다. 4) 두경부 영역에서 점액낭선암종은 전세계적으로도 매우 드물게 보고되며, 대부분 단일 사례로 보고된다. 5) 그 중에서도 구강 내의 점액낭선암종은 주로 주타액선에 발생하며, 소타액선에 발생한 점액낭선암종은 극히 드문 경우이고, 설, 구강저, 구개와 협점막 증례가 보고 되었다. 6) 저자들은 제 8번 흉추의 척추종양으로 진단되어 치료 중인 환자에서 우연히 발견된 상순 구순점막의 점액낭선암종 1예를 문헌 고찰과 함께 보고하는 바이다.
증례
78세 기저 질환 및 특이 과거력 없는 여자 환자가 3일 전부터 시작된 등 중앙부의 통증으로 타병원 의뢰 하에 내원하였고 자기공명영상장치(Magnetic Resonance Imaging) 검사 소견 상, 제 9번 흉추의 압박골절 및 제 8번 흉추의 경막내 종양 소견이 관찰되었다. 신경외과 치료 목적으로 국소 마취 하, 제 9번 흉추의 경피적 척추성형술(percutaneous vertebroplasty) 시행 받았다. 입원 당시, 환자는 상순의 구순점막에 위치한 구강 내 농양에 대해 불편감을 호소하여 성형외과로 의뢰되었다. 1년 전 동일 증상으로 타병원에서 절개배농술을 3개월 간격으로 2회 시행 받았으나, 재발되었다. 지난 9개월 동안 종물의 크기는 지속적으로 커졌다고 하였다. 종물의 크기는 직경 1cm의 원형 모양이었고, 점막 하에 위치하여 점막에는 0.2cm 직경의 구멍만 관찰되었다(Fig. 1). 경계가 명확한 매끄러운 표면의 돌출성 종물로 압통은 관찰되지 않았고, 압출 시, 장액성 분비물이 관찰되었다. 종양 감별을 위해 진단 및 치료 목적으로 수술적 절제를 결정하였다.

Pre operative findings. (A) 1×1cm round protruded mass was checked on labial mucosa of upper lip. (B) 0.2cm sized opening was checked on mass. (C) when squeezing, sticky discharge was checked.
수술 시 종물은 경계가 좋았기 때문에 깔끔한 박리가 가능했고, 수술 시 육안적 소견으로 남아있는 종물이 없도록 광범위 절제를 시행하였다(Fig. 2, Fig. 3). 절제한 조직을 병리조직검사 시행하였고, 절제연에 대해 조직간 층을 맞추어 봉합을 시행하였다. 병리조직검사 결과에서 종양은 다수의 낭포성 공간(cystic space)으로 구성되고, 이 공간 내로 세포질내 점액질(intracytoplasmic mucin)을 함유한 원주상피세포(columnar epithelial cells)가 관-융모상 성장(tubulo-villous growth)을 하고 있었다. 종양의 낭포성 공간은 대부분 둥글고 매끄러운 가장자리를 보였으나, 다수의 작은 부분에서 침윤성 성장을 보였다. 종양세포는 핵-세포질 비율은 낮았으나, 투명한 핵질과 분명한 핵소체를 보였고, 간혹, 핵분열도 관찰되었다(Fig. 4). 이와 같은 병리 소견상, 다른 장기에서의 전이를 배제할 수 있다면, 이 종양은 타액선 기원의 저등급 점액낭선암종에 합당 하였다. 이후 임파선 전이의 감별을 위해 두경부의 촉진을 시행하였고, 양측 하악각(mandibular angle) 위치의 2×2cm의 촉진되는 무통성 종물 소견이 관찰되었다(Fig. 5). 영상검사와 면역조직화학검사의 추가적인 검사를 계획하였으나 환자가 추가적인 치료에 대해 타병원 전원을 희망하여 추적 관찰이 불가능하였다.
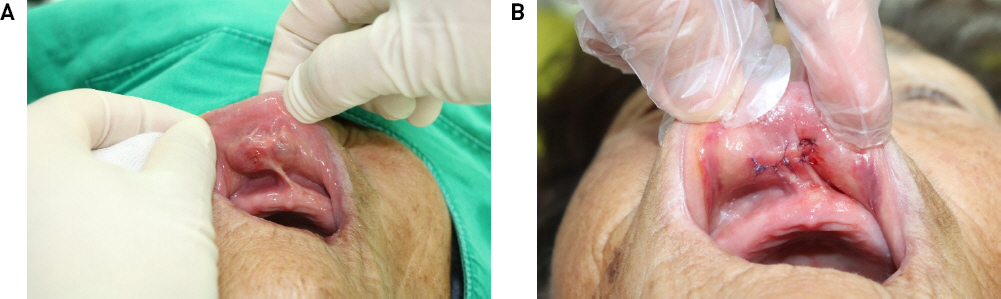
Intraoperative findings. (A, B) Wide excision and biopsy was done.

Gross findings. Received in formalin are 2 pieces of soft tissue, upto 1.1×0.6×0.4cm.
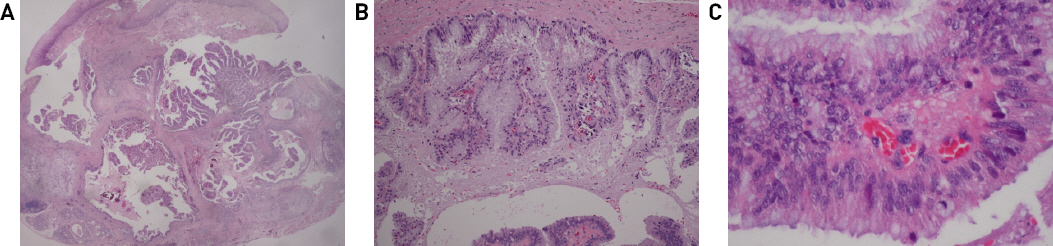
Histopathological findings. (A) (×12) The tumor is characterized by multiple cystic spaces with intraluminal, papillary growth of mucinous, columnar epithelial cells. (B) (×100) There is a cystic space with intraluminal papillary growth of mucinous, columnar epithelial cells. (C) (×400) The tumor cells show vesicular nuclei with distinct nucleoli & mitotic activity.

Postoperative findings. (A) Complete healing was checked and there was no recurrence until 2 weeks from operation. (B, C) 2×2cm sized palpated painless mass were observed at both mandibular angle.
고찰
점액낭선암종은 드문 암종으로 노인 여성에서 상대적인 발생 빈도가 높고, 주로 난소, 췌장 및 유방에 발생한다. 7) 그러나 점액낭선암종은 모든 선조직(grandular tissue)에서 발생이 가능하며, 특히 두경부 영역에서 발견된 점액낭선암종은 매우 드물다. 다른 분류로 모든 구강 내 타액선 종양의 10%는 선암종이며, 타액선 기원 선암종의 0.9%는 입술에 발생한다. 8)
점액낭선암종은 WHO에 의해 “papillary cystadenocarcinoma”로서 분류 기준에 포함되었고, 같은 해 the United States Armed Forces Institute of Pathology는 “cystadenocarcinoma with or without a papillary component”로서 분류되었다. 9) 대부분의 점액낭선암종은 주타액선, 특히 이하선에 발생하며 구강 내 발생 시, 공격적인 침범을 보이는 경우는 드물다. 5) 이 종양은 구강내 발생은 타 조직 기원의 종양과 조직학적으로 유사하며, 샘조직 패턴을 가지는 점막표피양 암종(mucoepidermoid carcinoma), 세엽세포암종(acinic cell carcinoma), 타액선관상피암종(salivary duct carcinoma), 비강샘암종(nasal adenocarcinoma) 그리고 전이성암종(metastatic carcinoma)와 같은 구강내 신생물과 감별이 필요하다. 1)
모든 형태의 입술 선암은 드물기 때문에, 이번 사례처럼 입술 점막에 발생한 점액낭선암종는 처음부터 악성 종물로 의심하기 어렵다. 이는 타액선 기원의 점액낭선암종은 선종, 섬유종 또는 화농성 육아종과 유사한 성장패턴을 보이고, 압출 시, 장액성 분비물 소견을 보인다는 점에서 점액낭포종으로 오인하기 쉽기 때문이다. 이번 사례의 환자는 1년 전 타병원에서 절개 배농술을 시행한 위치에 재발성 병변이 생긴 것으로 판단하여 펀치생검술(punch biopsy)를 고려하지 않고, 절제생검술(excisional biopsy)를 시행하였다.
조직검사는 종양의 정확한 진단을 위해 피부 병변의 일부 또는 전체를 채취하여 현미경을 이용해 검사하는 것으로, 임상적으로 흔히 사용된다. 펀치생검술은 두꺼운 병변에서 조직을 쉽게 채취 할 수 있고 상처가 거의 남지 않는 장점이 있지만 병변의 일부만 확인 할 수 있다. 절제생검술은 종양에 대한 전체를 채취해 진단과 치료가 한번에 가능한 장점이 있지만 흉터를 남길 수 있고, 결과에 따라 추가수술의 가능성이 있다. 이번 사례를 통하여 임상적으로 양성종양이 유력할지라도 펀치생검술이나 절제생검술을 이용한 조직검사를 반드시 시행할 필요가 있다고 생각된다.
타액선 기원의 점액낭선암종에서 원발성 기원과 전이성 종양의 감별진단을 위해서 방사선검사 및 면역조직화학 검사의 시행이 필요하다. 흉부, 복부, 골반의 컴퓨터 단층 촬영(computed tomography) 및 전신 양전자 단층 촬영(positron emission tomography)이 권장되며, 면역조직화학 검사에서 CK, CKH, CK8/18, CK7, CK19, S-100 그리고 Ki-67와 같은 표지자 들은 양성 반응을 보인다. 10) 다른 한편으로 ER 및 PR에 대한 반응성은 피부/유방 원발성을 강력하게 가리킨다. 11) 그러나 실제로, 최종 결정을 내리기 전에 임상 결과에 의존하는 것이 가장 중요하다. 더욱이 입술은 전이의 가능성이 떨어지는 부위이며 점액낭선암종의 입술 전이에 대한 설명은 문헌에 없다.
타액선 악성 종양의 발병률과 사망률은 인종과 성별에 따라 다르며, 백인 남성의 연평균 발병률은 인구 100,000명당 1.2명이고 흑인 남성의 경우 인구 100,000명당 1.0명이었다. 여성의 경우 두 인종 모두 인구 10만 명당 발생률이 0.7이고 남성의 유병률이 높음에도 불구하고 여성에서 높은 생존율을 보였다. 12) 특히 소타액선 기원 악성종양의 치료 후 재발의 70%가 초기 3년동안 발생하므로, 이 기간의 정기적인 경과 관찰이 중요하다. 13)
타액선 에서 발생한 발생한 점액낭선암종이 매우 극소수 이므로, 아직 정립된 치료 방법은 없지만 일반적으로 초기치료로 광범위 절제술 및 림프절 절제술을 시행한다. 방사선검사 및 면역조직화학 검사를 이용한 정기적인 경과 관찰 중 전이나 재발 암이 있는 경우 광범위 절제술 및 경부청소술(neck dissection)이 필요할 것으로 생각되며, 추가적인 항암화악요법 및 방사선치료를 수술 후 치료로 고려할 필요가 있다. 14)
Acknowledgments
This study was approved by the Institutional Review Board (IRB) of our medical institution (IRB No. KUCH 2020-11-033). This study conforms to the Declaration of Helsinki ethical principles for medical research.