경부에 발생한 지방모세포종 1예
A case of neck lipoblastoma in a pediatric patient
Article information
Trans Abstract
Lipoblastoma is a rare benign tumor with 80-90% occurring in children less than 3 years of age and 40% occurring in children less than 1 year of age. The most common site of incidence is limb, and then trunk. Neck is the rare site of incidence. The main symptom that the patient complains about is a rapidly growing neck mass without pain. When the size of mass increases, it can cause dyspnea, Horner's syndrome. Lipoblastoma is usually diagnosed as a lipoma in the fine needle aspiration. Since it is not differentiated from lipoma, liposarcoma, and hibernating adenoma in CT and MRI, the definitive diagnosis is histologic diagnosis through surgical resection. The treatment is complete surgical resection. And recurrence rate is 9-25% due to incomplete resection. Authors report this case with a review of literatures since we experienced a case of lipoblastoma diagnosed histopathologically after surgical treatment of neck mass.
서론
지방모세포종은 드물게 발생하는 양성 종양으로 80-90%가 3세 미만의 소아에서 발생하며 40%가 1세 미만의 소아에서 발병한다. 호발부위는 사지(30-70%), 몸통(20-50%)이며 경부에 발생하는 경우는 드물다[1,2].
환자가 호소하는 주된 증상은 통증을 동반하지 않는 크기가 빠르게 증가하는 경부 종물이다. 치료가 늦어질 경우 증가된 크기로 인해 주변 구조물을 압박함으로써 호흡곤란, 호너 증후군, 편마비가 발생할 수 있다[3,4].
저자들은 경부 종물을 주소로 내원하여 수술적 치료를 받은 후 병리학적으로 지방모세포종 진단된 환자 1예를 경험하였기에 문헌고찰과 함께 본 증례를 보고하는 바이다.
증례
한 달 전부터 시작되어 갑작스러운 크기 증가를 보이는 우측 경부 종물을 주소로 내원한 12개월 여자환자로, 진찰시 우측 경부의 5.0x4.0cm 크기의 부드럽고, 고정된, 압통을 동반하지 않은 종물이 확인되었다(Fig. 1A and B). 경부 전산화 단층촬영상 우측 악하부 피하지방층에 약 4.8x4.1cm 크기의 지방으로 이루어진 종물이 확인되었으며, 내부에 격벽 모양의 형태를 보이는 연부 조직 음영이 보이며 경계는 비교적 명확하게 보이고 있었다(Fig. 2A and B).
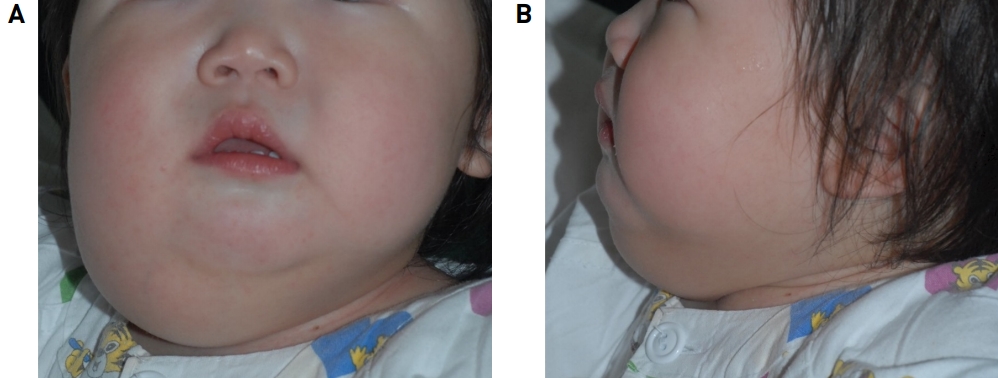
Preoperative findings. About 5.0 x 4.0cm sized, soft, fixed, nontender mass on right submandibular area in frontal view (A) and lateral view (B).
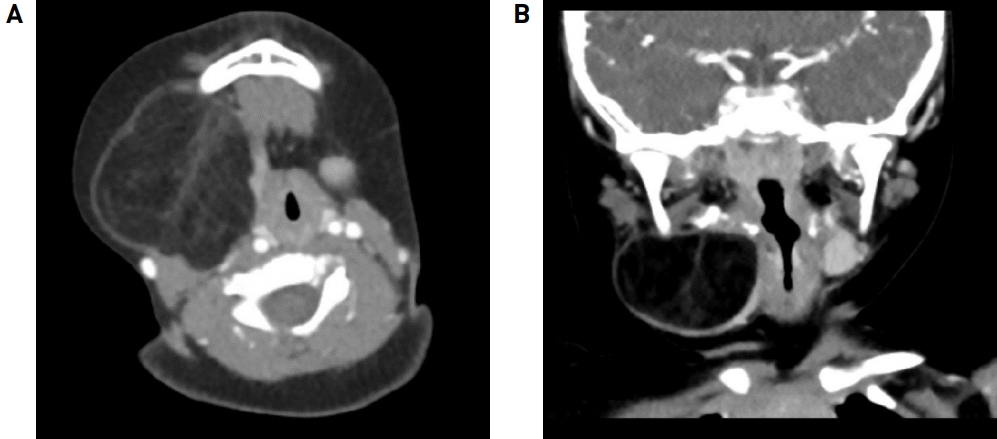
Enhanced neck CT scan reveals about 4.8 x 4.1cm size large fatty mass with septal like soft tissue density in right sub- mandibular area. Axial view (A) and coronal view (B).
상기 증상에 대하여 전신마취 하 우측 경부 종물에 대한 수술적인 절제를 계획하였다. 우측 하악 2cm 아래에 하악의 아래모서리와 평행한 절개선을 가한 후에 우측 악하부에 불규칙적인 모양의 피막이 잘 형성되어 있는 종물을 확인하였으며, 이를 완전히 절제한 뒤 수술을 마무리 하였다. 수술 후 약간의 수술 부위 통증 외 특이 호소 소견 및 합병증은 없었으며, 수술 후 2일째에 퇴원하였다.
절제된 조직의 크기는 6.5x4.7x3.5cm 였으며 육안적으로 부드러운 경계를 가지며 밝은 노란색을 띄고 있었다. H-E 염색상 절단면에서 창백한 빛깔을 띄고 있으며, 미성숙한 지방세포들의 소엽들이 확인되었다. 또한 단수 혹은 다수의 액포와 함께 얼기 모양의 혈관층을 갖는 지방모세포들을 관찰할 수 있었으며, 이에 지방모세포종으로 진단하였다(Fig. 3).

Pathologic findings. 6.5 x 4.7cm sized mass with smooth surface (A). On section, cut surface of mass shows pale appearance (B). Lobules of immature adipocytes (dotted arrow) separated by fibrous septa (black arrow) in a myxoid stromal background (Hematoxylin & Eosin, X100)(C). Lipoblastomas show univacuolar/multivacuolar lipoblasts (red arrow) and a prominent plexiform vasculature (Hematoxylin & Eosin, X200)(D).
수술 후 합병증 및 재발 소견은 확인되지 않았으며, 퇴원 후 약 2년간에 걸쳐 외래 추적 관찰하면서 촬영한 경부 전산화 단층촬영에서 재발이 의심되는 병변은 보이지 않았고 그 외에 특이소견은 확인되지 않았다. 이에 외래에 간헐적으로 내원하여 경과관찰 할 것을 권유하였다.
고찰
지방모세포종은 수술 전 시행하는 세침흡인검사에서 지방종으로 진단되는 경우가 대부분이며 전산화 단층촬영상 지방 조직과 같은 Hounsfield number 를 갖는 조영 증강 되지 않는 종물로 보인다[5].
감별해야 할 질환으로는 지방종, 지방육종, 동면선종 등이 있으며 이들 질환들은 전산화 단층 촬영 검사, 자기공명 영상, 초음파 검사와 같은 영상의학적인 검사로 명확히 감별할 수 없으므로 확실한 진단 방법은 수술적 절제를 통한 조직학적 진단이다[6]. 다만, 지방모세포종은 지방종과 달리 크기가 빠르게 증가하는 것이 특징이며 병력을 통해 의심해 볼 수 있다[7]. 최근 연구에 따르면 지방모세포종 환자의 약 70%에서 PLAG1 유전자의 재배열이 확인되며, 세침흡인검사와 형광동소부합법(fluorescent in situ hybridization)을 시행함으로써 이러한 유전자의 재배열을 확인하는 것으로 수술적 절제를 시행하기 전에 지방모세포종을 감별하는데 진단적인 도구로서 사용될 수 있다고 한다[8].
아직까지 자연적으로 감소한 증례가 보고된 바 없고, 경과관찰 할 경우 크기의 증가로 인한 다양한 임상 증상이 발생할 수 있다. 또한 피막이 잘 형성되어있고 주변 조직이 거의 없는 종양이므로 신경과 혈관을 보존하면서 완전한 수술적 절제를 시행하는 것이 치료 방법으로, 주변 또는 원격으로 전이는 하지 않는다. 다만 수술 후 불완전한 절제로 인한 재발율이 9- 25 % 정도로 문헌상 보고되고 있다. 따라서 수술적 치료를 시행한 뒤 정기적인 외래 추적 관찰을 통해서 종양의 재발을 확인하는 것이 바람직하다고 할 수 있다[9,10].
지방모세포종은 드물게 발생하는 양성 종양으로 주로 사지에 발생하며 경부에 발생하는 경우는 극히 드물지만 3세 미만의 소아에서 발생한 크기가 빠르게 증가하는 경부 종물에 대해서 지방종, 지방육종 등과 함께 감별진단에 고려해야 하며 수술적 치료를 포함한 적절한 치료방법을 결정하는 것이 바람직할 것으로 사료된다.
저자들은 경부에 발생한 지방모세포종을 절제한 보고가 드물고, 수술적 절제를 통하여 우연히 진단 및 치료하였기에 문헌고찰과 그 임상적 의의를 보고하는 바이며, 지방모세포종의 경우 지방종에 비해 짧은 기간에 빠른 속도의 크기 증가를 보이며 이에 따른 호흡 곤란 등의 중대한 합병증을 동반할 가능성이 있으므로 의심될 경우 빠른 수술적 치료가 필요하겠다는 교훈을 얻었다. 또한 세침흡인검사 및 형광동소부합법(fluorescent in situ hybridization) 등 술 전 지방모세포종을 감별할 수 있는 진단방법에 대한 추가 연구가 필요하다고 생각한다.