아랫입술의 편평세포암 환자에서 아랫 입술 폭 손실을 최소화하고 입벌림 기능을 보존하기 위한 새로운 점막지붕 피판 재건술
Mucosal Roofing Flap Reconstruction to Minimize Horizontal Lip Length Loss and Preserve Mouth Opening in Lower Lip Squamous Cell Carcinoma
Article information
Abstract
= Abstract =
Lower lip reconstruction in cases with a full-thickness defect over one-third of the vermilion is challenging. Numerous conventional techniques have been applied with unsatisfactory surgical outcomes because of microstomia and oral commissure blunting due to shortened horizontal lip length. Herein, we present a case in which a full-thickness lower lip defect of more than one-third of the horizontal lip length was covered with a novel mucosal roofing flap reconstruction to minimize the loss of horizontal lip length and to preserve mouth opening. No recurrences or metastases were observed during 3 years and 6 months of follow-up, with horizontal lower lip length maintained and mouth opening of 2.5 finger breadths.
Introduction
Squamous cell carcinoma is the most common malignant tumor related to the lips and occurs more frequently on the lower lip.1) The mainstay of treatment with regard to the lower lip lesion is wide excision with appropriate oncological safety margins and concurrent radiation therapy for advanced tumors.2,3) Numerous conventional reconstruction techniques have been applied based on the size and location of the defect.1,2,4) However, a wide resection including more than one-third of the lower lip often results in significant defects and may lead to microstomia with mouth opening impairment.5,6) Therefore, achieving the best functional and cosmetic results with primary resection and reconstructive surgery, as well as avoiding unnecessary secondary procedures, are of great importance to reconstructive surgeons. Herein, we introduce a novel lower lip reconstruction technique using a mucosal roofing flap to minimize the loss of horizontal lip length and mouth-opening impairment for defects of over one-third of the lower lip due to squamous cell carcinoma resection.
Case report
A 76-year-old male presented with recurrent ulcerative lesions on the right lower lip (Fig. 1). A punch biopsy by a dermatologist revealed squamous cell carcinoma. The patient had underlying stage 3 chronic kidney disease and cerebral infarction, but had never been diagnosed with cancer. On physical examination, the lesion (approximately 1.5 cm x 1.0 cm) had a central ulcerative surface with surrounding keratinization accompanied by pain and itching. After consultation with the Departments of Oncology and Radiation Oncology, staging and treatment plans were established. Contrast-enhanced neck computed tomography showed high-density at the level IB lymph node of the right neck and positron emission tomography-computed tomography revealed asymmetric F-18 fluorodeoxyglucose uptake at the same area; no other suspected lymph nodes or distant metastases were observed. Ultrasound-induced fine needle aspiration biopsy of this lymph node was performed, resulting in a diagnosis of reactive hyperplasia based on cytopathology.

Preoperative clinical photo of the squamous cell carcinoma on the right lower lip.
Thereafter, a wedge-shaped wide resection without lymph node dissection was planned, with a safety margin of 5 mm from the tumor edge. Intraoperative frozen section biopsy confirmed squamous cell carcinoma with tumor-free margins. Tumor resection resulted in a full-thickness lower lip defect (size, approximately 3.2 cm x 2.5 cm) that was more than one-third of the horizontal lower lip length (Fig. 2). As primary closure would have resulted in a loss of horizontal lower lip length, causing microstomia, a new flap surgery called “mucosal roofing flap” was performed. After undermining the submucosal plane in the inner aspect of the lower lip defect, a mucosal flap with minimal V-Y patterned inner mucosa was elevated. Thereafter, the flap was insetted and inserted into the red line between the wet and dry mucosa on the outer aspect of the lower lip defect in a roofing pattern (Fig. 3). Upon final pathological examination, the diagnosis was moderately differentiated squamous cell carcinoma without marginal invasion. The dimension of tumor was 1.0 cm x 1.0 cm x 0.5 cm (depth of invasion: 5 mm), and the pathological staging was determined to be T1N0M0, interpreted as stage I. The flap healed stably and without complications. Cosmetic outcomes were tolerable and without deformity of the oral commissure or vermilion border. Furthermore, mouth opening was maintained at 2.5 finger breadths at 3 years and 6 months postoperatively, with decent function preservation. The patient was satisfied with and well tolerated the postoperative appearance and function of the lower lip (Fig. 4).
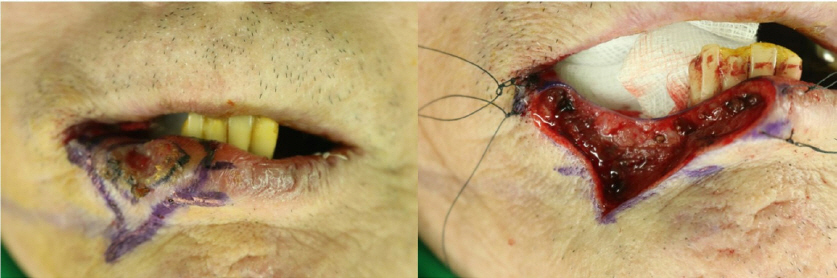
Intraoperative clinical photos. (Left) A wedge-shaped incision line is designed with a safety margin of 5 mm. (Right) The full-thickness lower lip defect of more than one-third of the horizontal lip length due to the wide excision is shown.
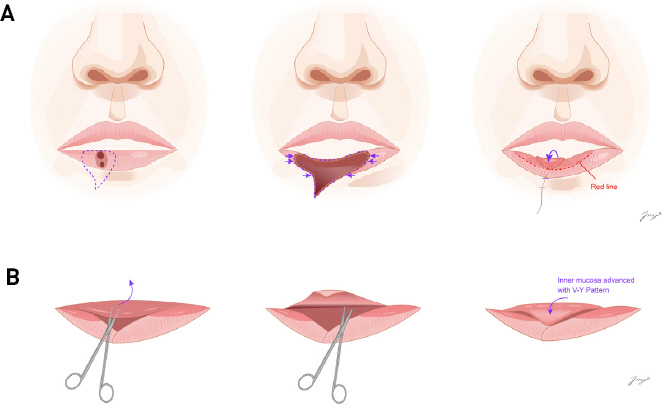
Depiction of the mucosal roofing flap. (A) After wedge-shaped wide excision, a mucosal roofing flap is elevated and advanced to the red line. (B) After undermining the submucosal plane from the inner aspect of the lower lip defect, the mucosal flap with minimal V-Y patterned inner mucosa was elevated. Thereafter, the flap is advanced to the red line in a roofing pattern.

Postoperative clinical photo at the 3 years and 6 months follow-up visit. Lower lip width and mouth opening are well maintained, without microstomia or oral commissure blunting.
Discussion
In general, the lip maintains the shape and symmetry of the aesthetic unit and plays major functional roles in verbal and emotional communication along with drooling prevention.7) The most common malignant tumor related to the lips is squamous cell carcinoma,1) which is most effectively treated by wide excision with appropriate margins. Numerous reconstruction techniques after resection have been reported for lower lip reconstruction, including primary closure; Karapandzic, Abbe, Estlander, and Bernard-Webster flaps; and their modifications or combinations.8-10) For full-thickness defects with a width between one-third and two-thirds of the lower lip, Karapandzic, Estlander and Abbe flaps have been mainly used. The Karapandzic flap, introduced in 1974, has the advantages of accurate visualization and preservation of the neurovascular bundles during flap dissection; however, it can lead to microstomia as the horizontal length of the lip is significantly decreased, and secondary commissuroplasty is necessary to correct microstomia in approximately 22% of cases.5,8,11) In addition, even when considering patients’ wrinkle lines and relaxed skin tension lines within aesthetic units, wide scars remain due to the extensive incision lines for the flap elevation. The Estlander flap is a single-stage lip-switch flap used for reconstructing oral commissure-involved defects. However, the Estlander flap requires frequent revision due to the occurrence of blunted obtuse angles at the oral commissure.8,12) As an alternative, the Abbe flap is used for covering upper and lower lip defects, replacing vertical height. However, the Abbe flap has the disadvantage of a lip adhesion period as well as causing imbalance between white roll and vermilion.8,13) In contrast, our novel flap technique provides better aesthetic and functional results in terms of inconspicuous scars, minimal donor site morbidity, and preservation of mouth opening. In addition, after undermining the submucosal plane from the inner aspect of the lower lip defect, the mucosal roofing flap was advanced and insetted and inserted into the border between the dry and wet mucosa of the lip to preserve horizontal lip length. Once microstomia occurs, patients suffer not only from cosmetic problems, but also from functional impairments such as difficulties in mouth opening and swallowing, poor oral hygiene, and speech disorders.14) However, our novel mucosal roofing flap technique could provide satisfactory surgical outcome in terms of preserving mouth opening over 2.5 finger breadths while minimizing the loss of horizontal lip length.
Conclusion
Our novel mucosal roofing flap may be considered as an alternative surgical option in cases of full-thickness lower lip defects of more than one-third of the horizontal lip length resulting from squamous cell carcinoma resection, preserving the lower lip length and minimizing the risk of microstomia.