후외측 목에 생긴 큰 규모의 근육간 지방종: 증례보고
A Large Intermuscular Lipoma of the Posterolateral Neck: A Case Report
Article information
Abstract
= Abstract =
Lipomas are a common soft-tissue tumor of mesenchymal origin, but intermuscular lipomas are very infrequently found especially in the cervical region. Although lipoma itself rarely causes complications, an accurate diagnosis and appropriate treatment are important. Surgical excision is indicated for deep lipomas that are 5 cm or larger, grow, or are accompanied by symptoms such as pain. It is also important to differentiate malignant tumors through pathological examination. Since the size of the lipoma was large, lipoma was divided into several pieces to successful removal, and the patient in this case showed successful recovery after surgery.
Introduction
Lipomas are a common soft-tissue tumor of mesenchymal origin.1-3) These tumors, which are composed of mature adipocytes, have been reported to be present in approximately 2% of the normal population. Clinically, it is a yellowish, painless mass that grows slowly and clearly demarcates the surrounding tissues.2-7) Intermuscular lipomas, which account for 0.3% of all benign tumors, are rare.3) Most intermuscular lipomas occur in the limbs, and they are very infrequently found in the cervical region.1) In this case report, we present a rare case of a large intermuscular lipoma on the posterior side of the cranio-cervical region, along with a review of the literature.
Case report
A 39-year-old man visited the Department of Plastic and Reconstructive Surgery for a lump in the posterior cervical region. The patient stated that the lump had formed 2-3 years ago and its size had increased over time (Fig. 1). The patient had no remarkable past medical history and indicated that he did not previously undergo surgery for the lesion because he thought it would disappear with time.

The picture above is a picture of a mass in the neck when the patient first came to the outpatient clinic.
A physical examination showed that the lesion was located in the right posterolateral part of the cervical region, with a maximum dimension of 10 cm. The patient complained of sporadic dull pain, and the lesion did not release any secretions upon pressure.
Preoperative computed tomography showed that in the right posterior lateral neck intermuscular space, there was a homogeneously hypodense lesion measuring approximately 10 cm that extended from the lower margin of the occipital bone to the level of the C5 vertebra (Fig. 2). A hypodense 6.0 × 5.0 cm mass was noted in the intermuscular space of the left neck, bordered by the splenius capitis muscle, levator scapulae muscle, and semispinalis muscle (Fig. 3).
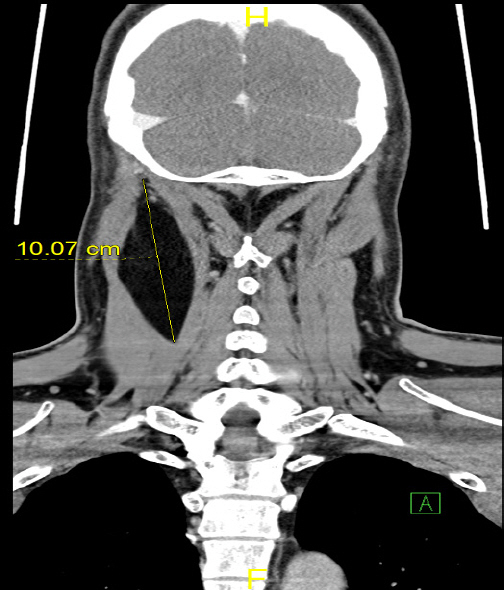
Preoperative computed tomography image. A hypodense 10cm mass is found in right posterior neck within right deep cervical muscles.
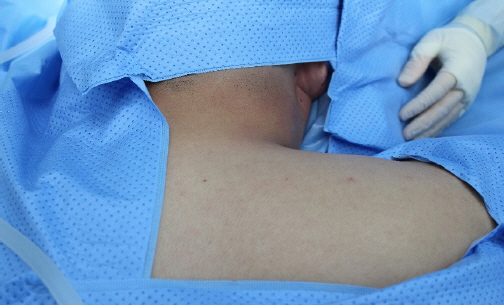
The picture above is a front view of the back of the patient’s neck before surgery. The patient was under general anesthesia.
A part of the mass was removed first and sent for a frozen biopsy, which confirmed that it was benign lipoma. The mass was then held with forceps or allis tissue forceps, split into pieces, and removed. Loose tissues around the tumor were easily separated from the surrounding tissues when they were desquamated and removed along with the lesion (Fig. 4). Surrounding structures such as the muscles and were not damaged during surgery, and after the mass was removed, each layer of the incised area was sutured. The operation ended after a Hemo-vac was inserted, and compressive dressing was performed to prevent seroma and hematoma. After surgery, the patient did not show any neurological symptoms such as cervical radiculopathy, nor did he complain of numbness or muscle weakness.

This is a photograph of a specimen obtained through surgical removal.
To limit the movement of the surgical site, the patient wore a neck collar for several days after surgery. The surgical site was checked for oozing or bloody discharge every day when it was being dressed. The wound healed without any remarkable symptoms or signs at 2-days later outpatient follow-up visits, and the patient no longer complained of the sporadic pain that he had experienced before surgery at 1 weeks later.
Discussion
A lipoma manifests as a lump with no significant effect on the human body. Histologically, it can be classified into simple lipoma, fibro-lipoma, spindle cell lipoma, intramuscular lipoma, cartilaginous lipoma, polymorphic lipoma, mucinous lipoma, and angiolipoma.8-9) Subcutaneous lipomas, which account for the majority of lipomas, generally present as lumps that do not meaningfully affect patients. However, they may grow over time and adhere to the surrounding tissues, causing pain or affecting movement. Despite the rarity of lipomas that occur in internal organs, an accurate diagnosis and appropriate treatment are important, as these lipomas may give rise to problems. In the present case report, a rare case of an intermuscular lipoma is described. The patient described herein had a 10-cm intermuscular lipoma located deep in the posterior cervical region, which has not been observed in previous cases. Surgical excision is indicated for deep lipomas that are 5 cm or larger, increase in size or are accompanied by symptoms such as pain.5) Lipomas 10 cm or larger were termed giant lipomas, and it was argued that if giant lipomas keep growing, the possibility of liposarcoma should be considered.6) Since the lipoma in this case report measured 10 cm and the patient complained of sporadic and dull pain, it was decided that surgical removal and histopathological testing were necessary to confirm whether the lipoma was malignant.4,5) Since it is difficult to remove a lipoma of this size as a whole, conducting a frozen biopsy first to confirm the positivity of the tumor and removing it in pieces can be proposed as a treatment method that does not result in damage to the surrounding tissues.10)
Intermuscular lipoma is located deep in the cervical region, the lipoma attached to the surrounding tissues should be removed slowly to minimize the possibility of post operative nerve damage or vertebral artery damage. a point to note is that when removing the mass in the intermuscluar space, it is recommended to perform surgery after accurately identifying the location of the mass from the occipital bone lower margin to the C-spine 5 level through Pharynx ECT. In the above case, the trapezius muscle lateral part was also approached, and intraoperative ultrasonography was also confirmed to find the mass of the cervical muscle deep layer.