

서론
전신 홍반 루푸스(Systemic lupus erythematosus, SLE)는 원인 미상의 전신 자가면역질환으로서 주로 젊은 여성에서 호발한다.1) 초기 증상으로 발열, 권태, 체중감소, 근육통, 관절통 등 비특이적인 증상에서 시작하여 피부발진, 구강궤양, 간비장 종대, 심막염, 늑막부종, 경부 종물, 발작, 뇌혈관계 질환 등의 다양한 임상양상을 보이며 특히 조혈계, 중추신경계, 심혈관계를 침범하였을 경우에는 사망에까지 이를 수 있다.2)
SLE에서 림프절의 침범은 12~59%까지 나타나는 비교적 흔한 임상 양상으로 그 중 24% 정도가 경부 종물로 발현하는 것으로 알려져 있고,3,4) 우리나라의 경우 2015년 기준 SLE의 유병률은 10만 명당 35.45명, 연간 발생률은 3.6명으로 추정된다.5) SLE는 비교적 젊은 연령대에 발생하여 만성적이며, 재발하며 진행하는 경과를 보이나 조기 진단과 코티코스테로이드, 면역억제제 등 치료법의 발달로 선진국에서는 10년 생존율이 95%이상으로 보고된다.6)
SLE는 이비인후과 영역에서 발열, 근육통 및 관절통 등으로 환자가 감기로 인식하여 내원하거나, 또는 경부의 종물로 발현되어 내원할 수 있으나 이러한 비특이적인 증상만으로 유병률이 낮으며 다양한 임상양상으로 발현되는 SLE를 의심하여 진단하기는 쉽지 않다. 저자들은 한 달 동안 지속되는 경부 종물을 주소로 내원한 38세 여환으로, 임상양상 및 혈액검사상 자가면역성 질환 의심하여 면역학적 검사, 조직 생검술을 통해 SLE로 진단한 1예를 경험하였기에 보고하고자 한다.
증례
환자는 이전 유산 과거력 있는 38세 여성으로 출산 2개월 후 발생하여 한 달 동안 지속되는 경부 종물로 내원하였다. 신체검사상 양측 경부 level I에서 각각 압통 동반하지 않는 부드러운 종괴가 크기는 우측 약 1 cm, 좌측 약 1.5 cm정도로 촉지되었고, 양측 손목 및 발목의 관절통 및 권태감 외에 다른 호소하는 증상은 없었다.
혈액검사에서 백혈구, 혈소판 수치는 정상이었으나 C-반응성 단백질(C-reactive protein, CRP)은 6.96 mg/dL으로 상승된 소견, 헤모글로빈(Hemoglobin, Hb)은 7.54 g/dL로 빈혈 소견을 보였으며, 상기 빈혈 소견은 임신 26주경부터 출산 시에도 확인된 소견이었다. 환자의 나이와 성별 및 무통성 경부 종물의 만성적인 양상을 고려하여 결핵성 림프절염과 CRP의 상승, 다발성 관절통, 지속되는 빈혈 소견 등에 대하여 Kikuchi병(Histiocytic necrotizing lymphadenitis, Kikuchi-Fujimoto disease), 자가면역성 질환의 가능성을 두고 경부 전산화 단층 촬영(Computed Tomography, CT), 세침흡입검사(Fine needle aspiration) 및 자가면역성 질환에 대한 선별 검사로 항핵항체(Antinuclear antibody, ANA) 검사를 계획하였다. 환자는 ANA 양성 소견을 보여, 류마티스 내과 의뢰하였고 추가적으로 시행한 면역학적 검사상 항지질항체(Antiphospholipid antibody), 이중나선 DNA항체(Anti-dsDNA antibody) 양성 소견 및 흉부 CT상에서는 양측 늑막 삼출 소견 보여 SLE의 진단 기준(Table 1)에 부합하였다.
Table 1
1997 American College of Rheumatology revised classification criteria for systemic lupus erythematosus [5]
류마티스 질환의 진단을 위해서는 불현성 감염, 악성 병변의 배제가 필수적이기 때문에 추가적으로 양전자방출단층 촬영(Positron emission tomography, PET) 시행하였고, 이전 시행한 경부 CT 상에서 관찰된 동일한 위치의 경부 level I, II, Va에 최대 2 cm 크기의 다수의 림프절들 뿐만 아니라(Fig. 1), 양측 액와, 후복막 및 양측 서혜부 림프절에서도 FDG 섭취 증가가 관찰되었다. PET-CT상 전신에서 관찰되는 다발성 림프절 비대에 대하여 악성 림프종을 배제하고자 기존 계획된 세침흡입검사 없이 국소마취하 좌측 level I의 경부림프절에서 진단적 목적의 절제생검 시행하였으며, 림프절은 직경 약 1.5 cm 크기 원형으로 주변 조직과의 유착이나 출혈 없이 원활히 박리되어 절제하였다.
Fig. 1
Radiologic imaging. Axial view of enhanced neck CT(A) and PET-CT(B) image show enlarged Neck Lymph nodes in both neck level II (arrow).

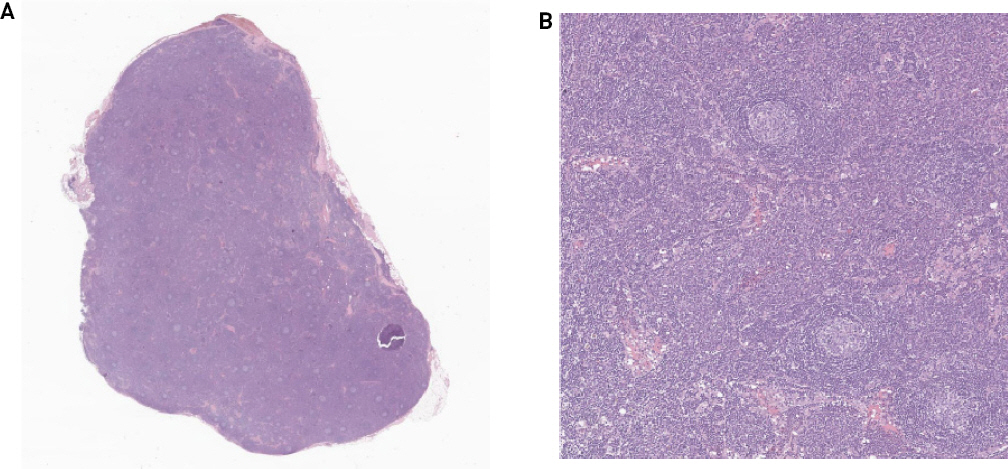
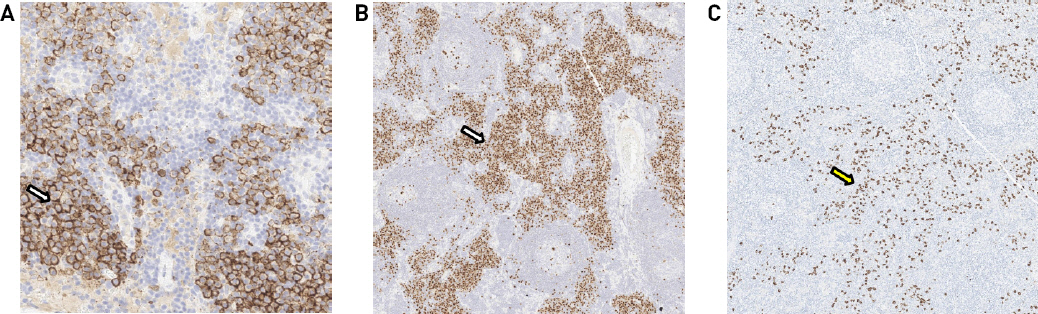
조직검사 결과상 림프절에 반응성 종자 중심(reactive germinal center)과 여포간 구역(interfollicular zone)에서 형질세포(plasma cell)의 침윤이 관찰되었고 이는 Kikuchi병 보다는 루푸스 림프절염을 시사하였다(Fig. 2). 면역조직화학염색에서는 다클론성을 시사하는 CD10, CD21, CD138, Ki-67, mun-1 과 IgG4에서 양성을 보여 자가면역질환의 특징을 보였으며(Fig. 3), CD3, CD20, 항산균(Acid fast bacilli, AFB) 염색에서는 음성소견을 보여 악성 림프종과 결핵 림프절염을 각각 배제할 수 있었다. 환자는 임상양상, 면역학적 검사, 영상학적 검사를 종합하여 최종적으로 SLE로 진단되었으며 주요 장기 침범이나 심각한 신체 증상 없어 류마티스 내과에서 약물로 증상 조절하며 정기적으로 외래 추적관찰 중에 있다.
고찰
경부의 림프절 종대는 이비인후과 의사로서 가장 흔하게 접하는 소견 중 하나로 반응성 림프절 종대(reactive lymph node hyperplasia)와 같은 비교적 경한 질환부터 악성 종양의 림프절 전이 또는 원발성 림프종 등의 중증 질환까지 매우 다양한 원인을 가질 수 있다. 실제 임상에서는 여러 검사에서도 특정 진단을 하기 어려운 림프절 비대 또한 드물지 않게 접하게 되는데, 특히 자가면역성 질환이 의심되는 경우에 진단은 한 가지 확실한 임상적, 방사선학적 또는 혈청학적 검사로 이루어지는 것이 아니라, 진단 기준에 따라 이 모두를 종합하여 이루어지며, 각각의 임상 증상에 대한 다른 질환의 배제가 필요하여 필연적으로 다양한 검사가 요구된다.
SLE는 젊은 여성에서 호발하는 전신 자가면역 질환으로 특징적으로 나비형 홍반(butterfly rash)부터 전신의 장기의 침범으로 간비종대, 사구체신염, 경련 등의 증상으로 다양한 임상양상을 보일 수 있는 내과 영역의 질환이나, SLE 환자에서 60%까지 림프절의 종대가 관찰되며 그 중 24% 정도가 경부 종물로 발현한다.3,4) 따라서 SLE가 초기에 경부 종물로 발현되는 경우 이비인후과를 내원할 수 있으므로 드문 질환이기는 하나, 이비인후과의사로서 의심하고 감별할 수 있어야 한다.
루푸스 림프절염에서 경부 림프절 종대의 경우 대게는 무통성으로 크기는 2 cm을 넘지 않으며,3) Kikuchi 병에서도 젊은 여성에서 비슷한 양상의 경부 종물과 드물지만 발열, 피부염, 관절염 혹은 간비종대 등이 동반할 수 있어7,8) SLE와 유사성을 보일 수 있고 실제로 오진되는 경우도 있다.9) 조직형태학적으로도 두 질환은 유사성을 지녀 일부 연구자들은 Kikuchi병이 루푸스의 전조 증상이라고 말하는 이도 있다.10,11) 하지만, 루푸스 림프절염의 경우 괴사부위를 형질세포가 둘러싸고 있고 헤마톡실린체(Hematoxylin body)들을 보이는 것이 특징으로 괴사 부위에 조직구나 단핵구 보다는 형질세포가 현저하고, 괴사 부위가 좀 더 광범위하다.7,12,13) 또한, Kikuchi병은 대부분이 혈청학적으로 항핵항체(ANA), 항 DNA 항체, 류마티스 인자(Rheumatoid factor) 등에 음성을 보이므로 루푸스 림프절염과 구별된다.14)
본 증례의 경우 무통성 경부의 림프절염과 다발성 관절통, 권태감과 함께 경부 림프절의 조직학적 검사결과를 통해 자가면역질환인 SLE와 Kikuchi병을 함께 의심할 수 있었다. SLE의 진단 기준에 부합하여 진단된 예로 과거 유산력과 항지질항체 양성 소견은 SLE에서 관찰 될 수 있는 소견이다.
이와 같이 SLE와 Kikuchi병은 임상적, 병리학적 유사성을 가지고 있으나 두 질환 간의 임상적 경과나 치료법은 큰 차이가 있다. Kikuchi병은 대부분 합병증 없이 자연 소실되며 대증적 요법으로 충분하나,15) SLE의 경우 경과에 따라 소염진통제부터 고용량의 스테로이드, 면역억제제가 필요할 수 있으며 적절한 치료 시기를 놓치면 사망과 같은 치명적인 결과에 이를 수가 있다.16)
SLE의 경우 현재로서 완치할 수 있는 방법은 없으나 선진국에서의 10년 생존율은 95%이상이 되는 질환으로, 이는 조기 진단 및 치료제 및 치료법의 발달로 기인한 것이다.17) SLE는 악화와 호전을 반복하며 만성적으로 지속되는 경과를 지니고 있어 조기 진단은 환자의 치료계획과 예후에 있어 매우 중요하며, 증상의 발현 후 진단이 빠를수록 루푸스 급성악화(SLE acute flare) 및 치료비용이 줄어든다는 분석결과도 보고된 바 있다.18)
따라서 젊은 여성이 만성적인 경과를 지닌 경부 종물로 내원하였을 때 Kikuchi병이나 우리나라에서 흔한 결핵성 림프절염 뿐만 아니라 이차적으로 구강궤양의 과거력, 안면의 피부 병변, 관절염 등 다른 전신 증상의 유무를 주의 깊게 확인하고 가능성이 있을 경우에는 전신홍반루푸스에 대한 선별검사로 자가항체검사를 시행하며, 필요에 따라 타 질환의 배제 또는 감별을 위하여 조직학적 검사가 필요할 것으로 사료된다.




