협점막에서 발생한 MALT 림프종 1예
A Case of Mucosa-Associated Lymphoid Tissue (MALT) Lymphoma in Buccal Mucosa
Article information
Abstract
= Abstract =
Extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue (MALT lymphoma) is a low- grade B-cell lymphoma that typically follows an indolent clinical course. It occurs in a variety of mucosal linings extranodal tissue, most commonly in the stomach. Other commonly involved sites include other parts of the gastrointestinal tract, thyroid, salivary gland, lung, lacrimal gland, synovium, dura mater, breast, skin, and eyes. It occurs very rarely in the buccal mucosa. A 50-year-old man came to the clinic while presenting a 5-month history of right- sided buccal mass. The incisional biopsy did not confirm the diagnosis of the lesion. He underwent complete excision of buccal mass for the diagnosis and treatment. The final pathology confirmed MALT lymphoma immunohistochemically. After surgery, he received radiotherapy with 30.6 Gy. There is no recurrence for 8 months after treatment. Herein we report a rare case of buccal MALT lymphoma with a review of the literature.
서론
림프종은 두경부 영역에서 편평상피세포암 다음으로 두 번째로 흔한 악성 신생물로, 두경부 전체 악성 종양의 5%를 차지한다.1) WHO 분류에 의하면 림프종은 면역표현형과 세포계열에 따라 호지킨 림프종과 비호지킨 림프종으로 분류한다.2) 호지킨 림프종은 경부 및 종격동 림프절 등 림프절을 주로 침범하며, 림프절 외 부위에서 발생하는 빈도는 1-4%이다. 그에 비해, 비호지킨 림프종의 40% 이상은 림프절 외 부위에서 발생한다.
점막 연관성 림프조직 림프종(mucosa-associated lymphoid tissue lymphoma, MALT lymphoma)은 B-세포 기원의 비호지킨 림프종의 아형으로 조직학적으로 저악성도의 B세포 림프종이다.3) 가장 호발하는 부위는 위이며, 그 외에 갑상선, 침샘, 편도, 비인두, 폐, 눈물샘, 활막, 경막, 유방, 피부 등 다양한 부위에서 발생한다.4,5)
구강에서 발생하는 림프종은 두경부 림프절 외 비호지킨 림프종의 0.2-3.0 %를 차지하며, 주로 구개에서 발생한다. 구강 내 특히 협부 점막에 발생하는 림프종은 매우 드물며, Silva 등은 구강에서 발생한 림프절 외 림프종 1289례 중 50례가 협부에서 발생하였다고 보고하였다.5) 국내에 보고된 두경부 영역의 MALT 림프종은 대부분 타액선 기원이었으며, 협부에 발생한 MALT 림프종은 2례가 보고된 바 있다.6,7)
이에 저자들은 50세 남자환자의 협부 점막에 발생한 MALT 림프종 1례를 경험하였기에 문헌 고찰과 함께 보고하고자 한다.
증례
50세 남자 환자가 내원 5개월 전부터 발생한 우측 협부 종물을 주소로 내원하였다. 과거 병력 상 특별한 내용은 없었다. 신체 검사상 우측 협부에 2.0x3.0cm 크기의 단단하고 주변 조직에 고정된 불분명한 경계의 궤양성 종물이 관찰되었다. 경부 전산화 단층촬영과 자기공명영상 상 상악후방의 지방조직으로 침윤되는 조영 증강 병변 및 동측 경부 level Ib에 림프절 종대가 관찰되었다(Fig. 1). 협점막암 의심 하에 협부 종물의 조직검사를 시행하였으나 심한 염증 소견만 관찰 되었으며, 우측 경부 level Ib림프절의 세침 흡인 세포검사에서는 반응성 림프절 과증식 소견 외 특이 소견은 없었다. 우측 경부 림프절은 경과 관찰 하기로 계획하였으며, 환자의 연령과 병변의 지속기간 등을 고려하여 절개 생검을 다시 시행하였고, 병리학적으로 림프종과 혈관염의 가능성 배제할 수 없다는 소견 외에 정확한 진단을 얻지 못하였다. 전신 양전자 방출 컴퓨터 단층촬영에서는 SUVmax 10.4의 고대사(hypermetabolic) 종괴 및 우측 경부 level Ib에 경부 림프절 종대 소견이 관찰되었다. 우측 협적막 종괴에 대한 정확한 진단 및 제거를 위한 수술을 계획하였다. 수술은 전신마취 하에 협점막 종물의 완전 절제를 시행 하였으며 종괴는 협부의 지방, 교근, 하악골까지 진행되어 있었으며, 종물 절제 후 결손 부위는 전층피부이식술로 재건하였다(Fig. 2).
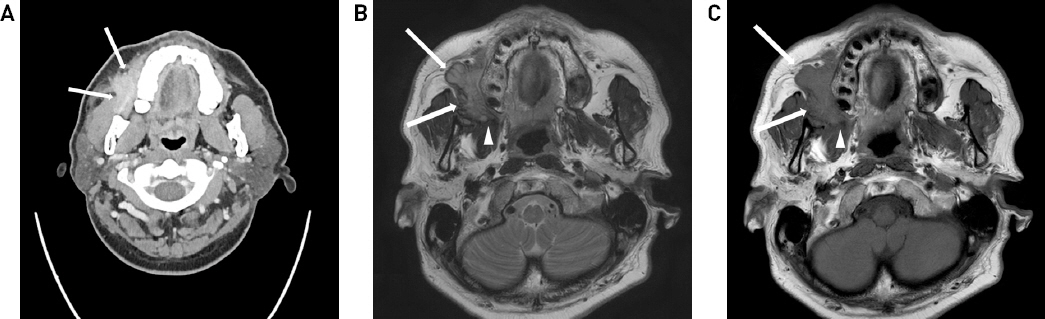
Imaging findings (A) An axial image of contrast-enhanced neck computed tomography shows an infiltrative well-enhancing mass (arrows) in the right buccal area extending to the buccal fat pad, the masseter muscle, and body of the mandible. (B and C) Axial T2-weighted (B) and T1-weighted (C) images of magnetic resonance demonstrate a well-circumscribed mass (arrows) extending to the retromolar trigone (arrowhead). The mass shows high T2 signal intensity and iso-intense T1 signal intensity compared to the surrounding muscle.
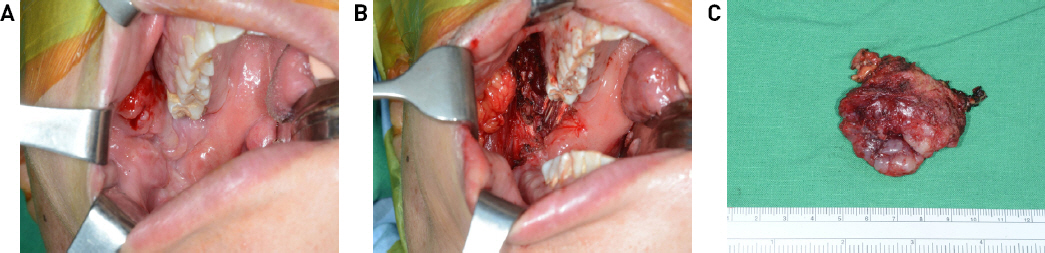
Operative view. (A) About 4cm sized hard mass is noted at the right buccal area. (B) The complete excision of buccal mass is performed. (C) The surgical specimen removed.
수술장에서 절제한 종물에 대하여 동결절편조직검사를 시행하였으나 정확한 진단은 불가능하였다. 최종 병리학적 결과에서 전반적인 림프구와 단핵구의 염증을 동반한 경화성 섬유증 및 실질의 상실이 관찰되었으며(Figs. 3A, 3B), 면역조직화학염색에서 B 림프구 표지자인 CD20에 강한 양성 반응을 보였고(Fig. 3C), T세포 표지자인 CD3에는 부분적으로 양성 반응을 보였다(Fig. 3D). Kappa 와 lambda의 light chain에 대한 in situ hybridization 검사에서 kappa chain에 대한 단일클론성 증식을 보였고, B-세포증식 질환을 시사하는IgH 유전자 재배열 검사 결과에서도 단일클론성이 확인되어 MALT 림프종으로 최종 진단되었다(Figs. 3E, 3F).
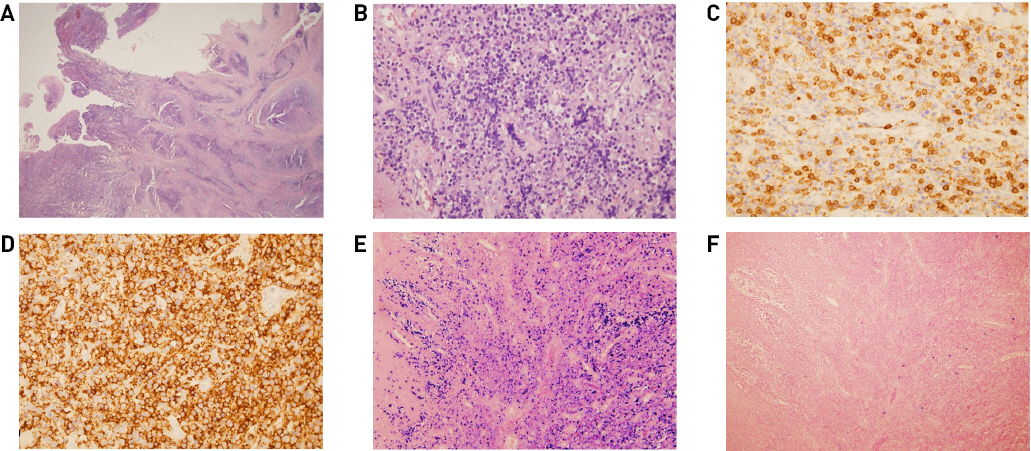
Pathologic findings. (A, B) Parenchymal fibrosis with lymphocytic and monocytic inflammation is noted in hematoxylin and eosin stain (H&E) staining (×12.5 (A) and x400 (B) magnification). (C, D) In immunohistochemical staining, atypical lymphocytes are diffusely immunoreactive for CD20, and few scattered cells are positive for CD3 (D). (E) In situ hybridization shows that atypical lymphocytes are positive for Kappa light chain (x400 magnification). (F) In situ hybridization for lambda light chain is negative (x400 magnification).
수술 후 협부 종양 부위에 30.6 Gy의 방사선치료를 시행하였고, 치료 후 8개월이 지난 지금 합병증이나 재발 없는 상태로 경과 관찰 중이다(Fig. 4). 술 전에 관찰되었던 우측 경부 림프절 종대 소견은 술 후 2개월에 시행한 경부 초음파 상 소실되었다.

The post-operative view of 8 months shows regression of the lesion and no recurrence.
고찰
두경부 영역에서 발생하는 MALT 림프종은 국소적인 종물과 통증, 구강내 궤양 형성을 보일 수 있지만 일반적으로 무증상으로 나타난다.8,9) 림프절 외 MALT 림프종은 헬리코박터균이나 EBV (Epstein-Barr virus)에 의한 감염 또는 쇼그렌 증후군과 하시모토 갑상선염 같은 자가면역과 연관되는 것으로 보아, 만성염증의 결과로 기원하는 것으로 여겨진다.10)
MALT 림프종의 영상 검사로는 전산화 단층촬영, 초음파 검사, 자기 공명 영상촬영, 동위원소 촬영 등이 이용되며, 영상학적 검사는 림프종 진단 후 병기를 결정하고 외과적 절제를 위한 계획을 세울 때 필요하나 MALT 림프종의 특징적인 소견은 없어 진단적 가치는 적다.
MALT 림프종은 조직병리학적 검사로 확진되며, MALT 림프종은 조직학적으로 중심세포양(centrocyte-like) 세포의 존재와 단핵구 모양 세포, 소림프구 등의 종양세포가 상피세포 내로 침윤하면서 형성된 림프상피성 병변의 형성과 형질세포의 분화 등의 소견을 보인다. 그러나 림프상피성 병변은 일반적인 염증 반응에서도 관찰될 수 있어 진단을 위해서는 면역조직화학적 검사가 필수적이다. 면역조직화학적 염색에서 MALT 림프종의 특이적인 표지자는 없으나, CD20, CD21, CD35, IgM(또는 IgA, IgG)에 양성이며, IgD에 음성으로 변연부 B 세포(Marginal zone B cell) 림프종의 면역표현형을 보이며, 여포성 림프종, 소림프구 림프종, 외투세포 림프종과의 감별을 위해 CD5, CD10, Cyclin D1 등의 염색에 음성 임을 확인 하여야 한다.10,11) IgH 유전자 재배열 검사는 림프종이 유전자 변형으로 인한 클론성 세포증식의 결과라는 점에서 면역글로불린 단일클론성 B 세포 증식을 확인함으로써 진단에 도움이 된다.11)
Suh 등은 MALT 림프종으로 최종 진단된 환자의 절반이 임상 양상과 세침 흡인검사에 의한 초기 진단에서 염증성 병변으로 오인되었다고 보고하였으며, 생검에서 면역조직학적 검사와 유전자 재배열 분석을 하여야 정확한 진단이 가능함을 강조하였다.12) 본 증례의 경우도 진단을 위해 반복적으로 절개 생검과 완전 절제술을 시행하였으며 면역조직화학염색법과 IgH 유전자 재배열 검사를 통해 림프종으로 확진 되었다.
MALT 림프종은 진행이 느리며 대부분의 경우 발생한 원발 부위에 국한되나, 병기 설정을 위해 경부, 흉부, 복부 전산화 단층촬영 및 골수 생검이 필요할 수 있다. 병기 결정은 병소의 해부학적 위치에 기초를 둔 Ann arbor를 따르며, 호지킨 림프종과 달리 비호지킨 림프종의 경우 병소의 병기 외에도 림프종 세포의 조직학적 분류가 예후에 영향을 미친다.10)
구강 MALT 림프종의 경우 명확한 치료 원칙은 없으나, 저등급의 국소 병변의 병기 I, II 기에서는 방사선 단독 요법이 선호되나, 원발 부위에 국한된 병변이거나 진단을 위한 수술적 절제를 고려할 수 있다. 다발성이거나 파종성으로 진행된 병기 III, IV 기의 치료로는 복합 항암화학요법을 시행하거나 추가적인 방사선 치료를 시행한다.9,12,13,14)
MALT 림프종의 예후는 5년 생존율이 75%로 다른 림프종과 비교하여 좋으나, 장기간 경과 뒤에도 재발 가능성이 높아 지속적인 추적 관찰이 요구된다.12)
결론적으로, 본 증례에서의 교훈은 오래 지속되는 협부 점막의 병변이 있을 때, MALT 림프종을 포함한 비호지킨 림프종의 가능성을 고려해야 하며, 조직학적 진단이 어려운 경우 수술적 절제를 통한 확진이 필요할 수 있다는 점이다.