증례보고: 이하선에 발생한 다형선종 유래 피막내 암종 1예
Case Report: Intracapsular Carcinoma Ex Pleomorphic Adenoma of Parotid Gland
Article information
Abstract
= Abstract =
Among a variety of malignant types for parotid gland tumors, intracapsular carcinoma ex pleomorphic adenoma which is classified as a non-invasive tumor has been reported rarely. We report a case of a 69-years old patient, who presented with a left parotid mass that was detected 30 years ago. Fine needle aspiration biopsy result of the mass was “suggestive of pleomorphic adenoma”. Superficial partial parotidectomy was performed for the mass and the permanent pathologic finding was “intracapsular carcinoma ex pleomorphic adenoma” which was a salivary ductal carcinoma with well-preserved myoepithelial cells surrounding the malignant epithelial cell clusters. Surgical resection is the main treatment modality for the treatment of intracapsular carcinoma ex pleomorphic adenoma. Herein, we present the case with a review of literature.
서론
다형선종 유래 암종(carcinoma ex pleomorphic adenoma)은 다형선종에서 발생하는 악성 종양으로 침샘에서 발생하는 악성종양의 약 12%를 차지한다.1,2) 이는 60-70대에서 가장 발병율이 높으며, 다형선 선종(pleomorphic adenoma)이 발병한 후 약 10-20년 이후에 가장 많이 발생한다.1,2)
다형선종 유래 암종은 악성 성분의 피막(capsule), 피막외 침범 정도에 따라 비침습(non-invasive), 미세 침습(minimally invasive), 침습(invasive) 다형선종 유래 암종으로 분류되는데 이는 예후와 관련이 깊다.3) 다형선종 유래 피막내 암종(intracapsular adenoma ex pleomorphic adenoma)은 병리학적으로 매우 드물게 보고되며 악성 성분이 다형선종의 피막 내부에서 관찰되어 다형선종 유래 암종 중 비침습 암종에 속한다. 악성 성분이 피막 내에 있으면 예후가 양성혼합종양(benign mixed tumor)와 다르지 않지만, 피막외로 침범한 경우에는 안 좋은 예후를 가지며, 약 25%에서는 주변 림프절 전이가 발생한다.4,5) 이러한 이유로 다형선종 유래 피막내 암종은 주변 조직으로 침윤과 다른 장기로의 전이가 없다고 알려져 왔으나, 조직학적으로 전이가 밝혀진 경우도 아주 드물게 보고되기도 했다.6,7)
최근 저자들이 경험한 69세 남자 환자의 경우 좌측 재발성 이하선 종물에 대해 시행한 세침흡인검사에서 다형선종으로 의심되어 수술하였고, 수술 후 병리조직 검사에서 다형선종 유래 피막내 암종으로 진단되었다. 아직까지 국내에서 해당 증례가 보고된 적이 없기에 문헌 고찰과 함께 보고 하고자 한다.
증례
69세 남자 환자가 35년 전 발생한 좌측 이하선 종물을 주소로 내원하였다. 타원에서 제거 수술을 받은 후 양성 종양 소견이었다고 하며, 약 30년 전부터 다시 좌측 이하선에 종물 만져졌으나 별다른 치료 없이 경과 관찰하다가 1년 전부터 크기가 증가하는 양상으로 본원 이비인후과에 내원하였다.
신체 진찰에서 좌측 이하선 부위에 약 5cm의 무통성의 단단한 종물이 관찰되었고, 종물은 고정되어 있지 않고 가동성이 있었다(Fig. 1). 종물 이외에 안면마비같은 동반 증상은 없었다. 술 전에 시행한 초음파 유도 하 세침흡인세포검사에서 비정형 세포들이 관찰되며 다형선종 의심(suggestive of pleomorphic adenoma)으로 보고되었다.
5cm sized mass was noted at left infraauricular region.
이하선 종물에 대한 영상학적 평가를 위해 경부 전산화 단층촬영(CT) 및 자기공명영상 촬영(MRI) 촬영했고, CT에서 좌측 이하선 천엽에 0.7-2cm가량의 종물들이 다수 확인되었고, 석회화 소견은 없었다(Fig. 2). T2강조 MRI에서 강한 조영증강, T1강조 MRI에서 약한 조영증강 소견으로 이하선 종물은 피부에 근접하여 피하층까지 침범해 있었다.
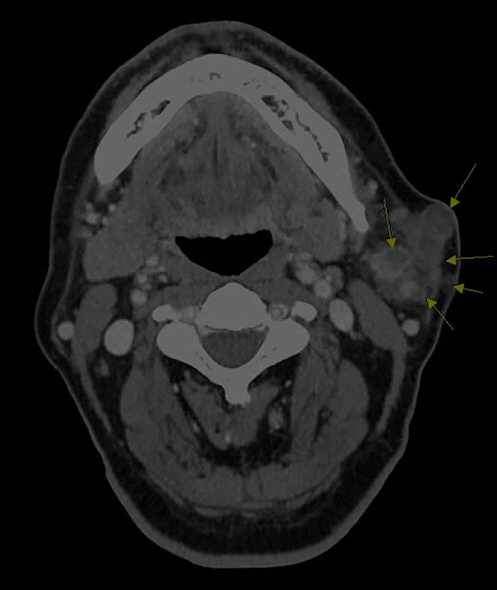
In enhanced neck CT, multiple conglomerated masses (7mm-2cm sized) without calcification were seen at the superficial lobe of left parotid.
환자는 전신마취로 앙와위 자세에서 안면신경 감시(nerve integrity monitoring; NIM-response 3.0 system, Medtronic, Jacksonville, FL, USA) 하 이하선 천엽절제술(superficial parotidectomy)을 시행받았다. 좌측에 변형 블레어 절개(modified Blair incision)를 가한 후 조직을 박리했다. 수술 중 좌측 천엽 전 측에 둥글게 덩어리진 종물들이 파하층까지 침범해 있었고, 안면신경의 경분지는 종물 사이로 관통하고 있었다(Fig. 3A). 안면신경의 주줄기(main trunk) 및 다른 분지들을 잘 박리하여 보존된 채 이하선의 종물들을 포함한 천엽을 깨끗하게 절제했다(Fig. 3B).
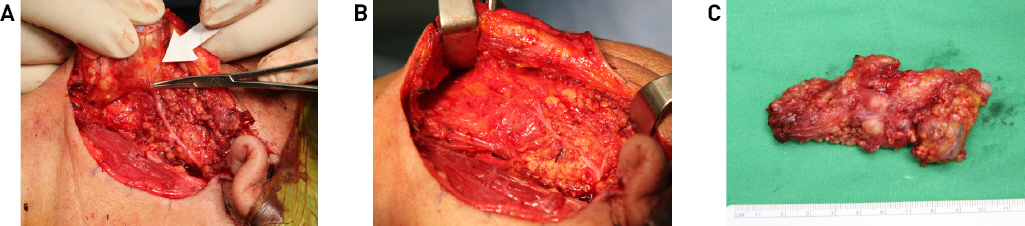
A. About 6.0 x 3.0 cm sized specimen was composed of conglomerated multiple masses. They were noted at the superficial lobe of left parotid gland. Anterior portion of the mass was extended to the subcutaneous space nearly abutting the skin. Cervical branch of the facial nerve was directly penetrating the mass. B. Branches of facial nerve except the cervical branch and the main trunk of the facial nerve were well identified, carefully separated from the mass, and were well preserved. C. Parotidectomy specimen. 6 X 3 X 2 cm tumor.
술후 병리조직검사에서 다형선종 유래 피막내암종으로 보고되었다. 절제된 검체는 6 x 3 x 2cm의 종양을 포함했다(Fig. 3C). 병변은 다결절성으로 경계는 명확했다. 종양의 절단면은 점액질(myxoid)에서부터 섬유질(fibrous)까지 불균질한 모습이었다. 종양에는 2.5cm의 악성 성분를 포함하고 있었는데, 이는 고도의 비정형 세포들로 구성되어 있었다.
수술 후 재원기간 동안 특별한 합병증 없었으며, 안면신경 장애는 관찰되지 않았다. 수술 10일 뒤 촬영한 전신 양전자 단층촬영(PET-CT) 검사에서 주변 경부나 다른 장기로의 전이소견은 없었다. 환자의 향후 치료방향 결정을 위해 이비인후과, 방사선 종양학과, 병리과, 영상의학과, 핵의학과의 의사들이 참여한 다학제 진료를 시행했고, 수술 후 방사선 요법을 포함한 추가 치료는 시행하지 않고 경과관찰 하기로 결정했다. 수술 후 6개월 간의 추적관찰 중 CT에서 확인된 재발소견은 없다.
고찰
해부학적으로 이하선은 침샘 종양의 가장 흔한 부위로, 침샘 종양 약 80~85%를 차지한다.3,8) 이러한 이하선 종양의 약 75%는 양성 종양이고 약 25%는 악성 종양이다.9) 다형선종 유래 암종은 원발성 또는 재발성 양성 다형선종에서 발생하는 암종으로 정의된다. 이는 침샘에 발생하는 악성 혼합종(malignant mixed tumor)중 한 분류로, 1.9~23.3%의 다형선종이 악성 종양으로 변하는 것으로 알려져 있다.4,10) 조직학적으로 침샘관 암종(ductal carcinoma)과 근상피 암종(myoepithelial carcinoma)은 다형선 유래 암종에서 가장 흔하게 관찰되며, 이외에도 상피-근상피 암종(epithelial-myoepithelial carcinoma) 및 편평세포 암종을 포함하여 다양하게 보고된다.11)
다형선종 유래 암종은 예후에 따라 비침습, 미세침습, 침습성 종양으로 분류할 수 있는데 기준은 악성 성분의 피막, 피막외로의 주변 조직 침범 정도이다. WHO기준에 따르면 다형선종 내의 악성 성분이 1.5 mm 이내의 피막외 침범을 보이면 비침습, 미세침습 종양이라 하고 1.5 mm 이상의 피막외 침범이 있으면 침습 종양이라 한다.3) 이 기준은 최근 연구들에 따라 완화된 기준으로 보아야 한다는 의견들도 있는데, 암성 성분이 피막외 조직으로 4- 6mm까지 침범해도 수년간 재발이 없어 미세침습 종양으로 분류할 수 있다는 보고들이 있다.12,13) WHO 분류에 따르면 다형선종 유래 피막내 암종은 다형선종에서 다형선종 유래 암종으로 진행하는 과정 중 한 단계로 기술되어 있으며, 피막외 침윤이 없기 때문에 좋은 예후를 갖는 것으로 보고되어 왔다.3,12,13) 본 증례의 경우 수술 후 병리조직검사에서 악성 성분이 피막내에 완전히 둘러싸인 다형선종 유래 피막내 암종으로 피막외 다른 조직의 침윤이 전혀 없는 비침습 암종으로 확인되었다.
WHO 분류에 따르면 다형선종 유래 피막내 암종은 다형선종에 있는 침샘관 내부 또는 침샘관들 사이에서 비정상적인 증식이 일어나는 것으로 정의한다.3) 대부분은 침샘관 암종으로 악성 성분이 내강 형태(luminal phenotype)로 나타나며, 다른 일반적인 표현형으로 근상피 암종이 있는데 이는 비내강 형태(abluminal phenotype)이다.1) 침샘관 암종의 표현형에서 내강 세포의 비정상적인 증식은 침샘관내에 국한되는데, 이러한 비정상 내강 세포들은 면역조직화학 분석에서 높은 Ki-67 및 Cytokeratin7, CK18가 발현되며 핵 비대 및 현저한 핵소체(nucleoli), 세포군집(cellular crowding), 빈번한 유사분열(mitosis)을 포함한 고등급 비정형성(high grade atypia)을 보인다. 기존에 있던 다형선종의 관들은 주변의 비내강 세포들(abluminal cells)에 의해 둘러싸여 있는데, 근상피 세포들을 포함한 비내강 세포들에서는 CK14, p63, SMA가 발현된다.1,13)
본 증례의 조직에 대한 면역조직화학 검사에서 악성 상피 세포는 Cytokeratin 7에 대해 양성이었고 높은 Ki-67 표지 지수를 나타내어 침샘관 암 성분임을 시사했다(Figs. 4A-4D). P63 및 평활근 액틴(smooth muscle actin, SMA)에 양성으로 표지 되는 근상피 세포들은 보존 되어있는 상태로 악성 상피 세포 군집을 잘 둘러싸고 있었는데, 이는 악성 세포 군집이 관내암종(intraductal carcinoma)임을 시사하는 소견이었다(Figs. 4E, 4F). 악성 종양의 인접 조직 침윤은 관찰되지 않았고, 림프관 침윤 및 신경주위 침윤도 관찰되지 않았다. 절제된 검체 중 악성 성분을 제외한 부분은 양성 낭종과 땀샘이 있는 다형선종으로 구성되어 있었다(Fig. 4A).
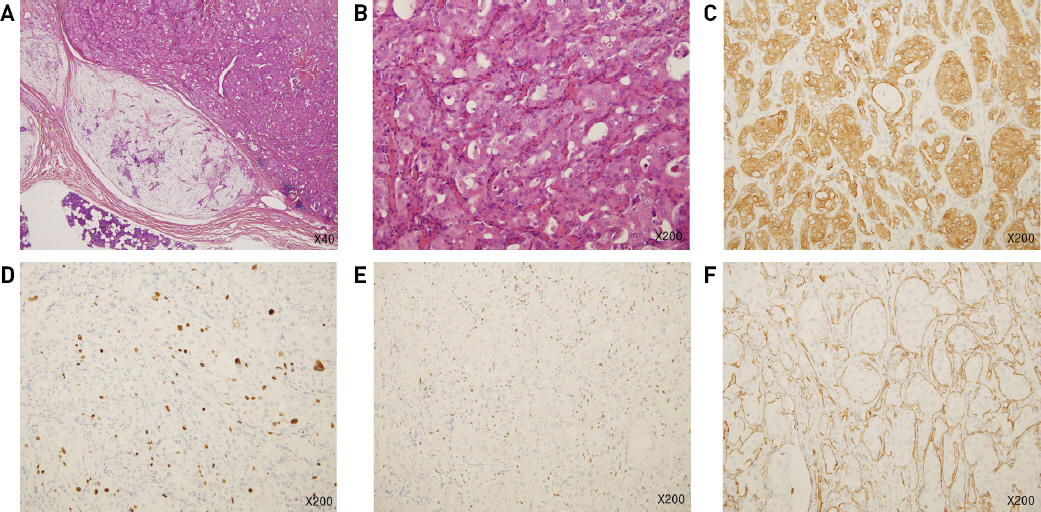
A. Low power view (x40) of the malignant component. The malignant component (upper right) is well demarcated from surrounding benign tissue. B. High power view (x200) of the malignant component. The lesion shows prominent cytologic atypia. C. IHC stain for cytokeratin 7 (x200). D. IHC stain for Ki-67(x200). The lesion shows high Ki-67 index. E. IHC stain for P63 (x200). F. IHC stain for SMA (x200). Well preserved myoepithelial cells are highlighted by P63 and SMA IHC stain.
원발성 또는 재발성 다형선종, 대부분의 침샘 암종에 대한 치료 원칙은 외과적 완전 절제이다. 침샘 암종의 경우 필요시 수술 후 방사선치료를 추가한다. 이하선 천엽 절제술은 이하선에서 발생하는 다형선종에 대한 수술적 치료의 좋은 선택이다. 종양만 단순 적출하는 경우 재발률은 20~45%이며 이하선 천엽 절제술로 재발률은 5% 미만으로 감소한다.14) 대부분의 다형선종의 경우 이하선 전절제술 같은 광범위한 절제가 재발 위험을 감소시키지 않으며, 오히려 안면 신경 기능 장애 및 기타 합병증 비율을 높이는 것으로 알려져 있다.14,15) 이하선 천엽에서 발생하는 초기의 저악성도 암종에도 이하선 천엽절제술을 시행한다.
선행 연구들에 따르면 다형선종 유래 피막내 암종(비침습성)은 수술적 절제만으로도 좋은 예후를 보인는데, Brandwein et al.의 보고에서 12명의 비침습성 또는 최소 침습성(<1.5mm) 다형선종 유래 암환자들에게 수술(이하선 천엽 절제술, 악하선 절제술)만 시행했고 13년간의 추적 기간내 재발이나 전이는 없었다.16) 비슷하게 Lewis et al.의 보고에서 수술적 치료를 받은 4명의 다형선종 유래 피막내 암환자들을 14개월에서 17년까지 추적 관찰한 결과 재발 소견은 없었다.1) 하지만 비침습성 다형선종 유래 암종이 완전히 전이 가능성이 없는 것은 아니다. Felix A et al.는 림프절 전이 동반된 다형선종 유래 피막내 암종의 사례를 보고한 바 있다.6)
본 증례의 환자는 35년전 발행한 좌측 이하선 종물에 대해 타원에서 종양만 단순 적출하는 수술을 받은 후 재발하여 약 30년이 지났다. 원발성 다형선종의 불완전한 절제로 재발성 다형선종이 발생한 것으로 판단된다. 또한 이환 기간이 약 30년이 지나 악성 변화가 발생하기 충분한 시간이 된다. 수술 전 시행한 세침흡인검사에서 다형선종이 의심되어 종양을 포함한 이하선 천엽절제술을 시행했고, 병리조직검사에서 악성 종양으로 확인되었지만 주변조직, 신경, 혈관, 림프관 침범이 없어 추가 방사선 치료는 하지 않고 추적 관찰하기로 했다. 수술 후 6개월째 CT 촬영을 포함한 추적관찰에서 재발 소견은 없다. 하지만 피막을 침범하지 않은 비침습 다형선종 유래 암종에서 림프절 전이가 확인된 증례도 보고된 만큼,6) 향후 면밀한 추적관찰이 필요할 것으로 보인다.