

Introduction
Schwannomas are slow-growing benign tumors of neuroectodermal origin that are derived from Schwann cells in the peripheral cutaneous or muscular branches of cranial or autonomic nerves. 1) These tumors can arise in any part of the body but rarely involve the auricle. Dokania et al. summarized the details of 9 cases from the English literature in tabular form. 2) The chief complaint was a painless mass in 8 of these cases. Therefore, cosmetic concerns may be more significant than neurologic symptoms in auricular schwannoma. However, when we reviewed these 9 cases of auricular schwannoma, 8 did not mention the cosmetic outcome.
Here we present a case of auricular schwannoma with a review of the literature and describe the surgical technique used from a cosmetic perspective.
Case Presentation
A 39-year-old woman was referred to our hospital to discuss the aesthetic management options for an asymptomatic mass in her left auricle that had developed over 2 months. There was no remarkable medical or family history. Physical examination revealed a firm, oval, well-circumscribed, non-tender mass with a diameter of 1 cm in the superior concha of the left auricle that was covered with normal skin (Fig. 1). Due to its small size, it was difficult to determine if the mass was adherent to surrounding structures, such as skin or cartilage. The mass had a peduncle that seemed to be in the inferior crus and was mobile. The differential diagnosis included epidermoid cyst, hypertrophic scar, and keloid.

The lesion was completely excised under local anesthesia. We planned preoperatively that the wound would be closed using the skin flap overlying the mass. The incision line was designed to run along the neck of the mass in a posteriorly half-circled manner to keep a pedicle for the flap (Fig. 2A). Intraoperatively, the mass was easily dissected from the underlying perichondrium and the overlying skin flap (Fig. 2B). Primary closure was performed by suturing the skin flap that previously covered the lesion (Fig. 2C). Compression gauze with tie-over sutures was applied between the inferior crus and crus helix (Fig. 2D). The tie-over sutures were removed on postoperative day 6. The final result was favorable with a viable skin flap (Fig. 3).
Fig. 2
. (A) The skin incision line was designed to run along the base of the mass (indicated by the solid red line) while avoiding the anteriorly based pedicle. (B) The mass (indicated in red) was dissected and the overlying skin flap was carefully and atraumatically retracted. (C) Primary closure was performed by suturing the overlying skin flap. (D) A tie-over dressing was applied to compress the skin flap onto the perichondrium.1,2)
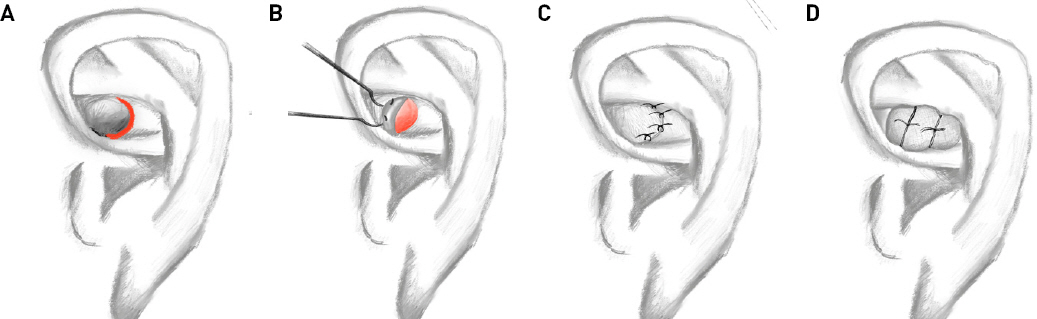
Fig. 3
Clinical photograph taken on postoperative day 14 showing a viable skin flap with an acceptable aesthetic outcome.

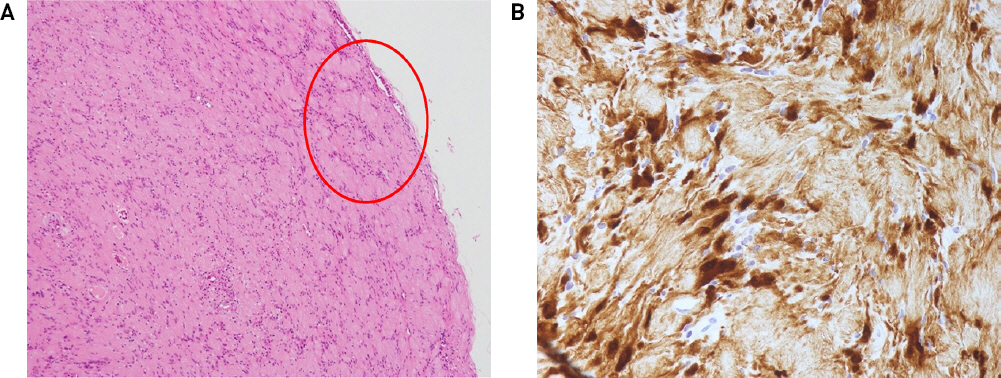
Gross examination revealed a 10 × 8-mm well-encapsulated oval mass with a smooth surface (Fig. 4). The pathology report noted an Antoni A area composed of spindle cells with nuclear palisading and Verocay bodies (Fig. 5A). Immunostaining was positive for anti-S100 protein and negative for alpha-smooth muscle actin (Fig. 5B). The final diagnosis was schwannoma. The gross anatomical location of the mass indicated that it originated from the auriculotemporal nerve. However, there was no abnormal sensation in the area supplied by this nerve after the excisional procedure. There have been no signs of local recurrence as of 10 months after surgery, and the patient has not complained of abnormal sensation around the auricle or any cosmetic concerns during this time.

Discussion
Schwannoma was first reported in 1910 by Verocay 3) and is a benign neoplasm derived from the Schwann sheath. 4) This tumor can arise in any area in the body innervated by a peripheral nerve that contains Schwann cells. 5) The most common extracranial sites are the head and neck. 6) The external ear is rarely involved, with most developing in the external auditory canal. 2) Tumors in the auricle are even rarer. 2) Patients with a tumor in the external auditory canal typically complain of hearing problems whereas those with auricular tumors are more likely to have cosmetic concerns. 7,8) To our knowledge, only 9 cases of auricular schwannoma have been reported in the English literature. The concha was the most commonly involved auricular site in the reported cases, as in our case, where the superior concha was affected. 2)
Jung et al. reported that the most common benign neoplasms in the auricle were epidermal cysts and that the lobule was the most frequently affected site. 9) In this case, our initial impression was also that the lesion was an epidermal cyst. Preoperative investigations indicated that the lesion was benign and easily anatomically approachable. Therefore, no additional radiological examinations were performed. However, the intraoperative findings were typical for schwannoma, so we believe that this mass was very unlikely to be an epidermal cyst.
Tsai et al. reported that extracranial schwannomas have a recurrence rate of 1.4%. 10) Given that these tumors commonly affect patients in their 20s, 30s, and 40s, consideration should be given to not only neurologic symptoms associated with the nerve involved or recurrence 5 but also the aesthetic outcome. The auricle is composed of cartilage and skin and has a complicated three-dimensional structure. 11) The convex and concave structures of the auricle need to be preserved and the surgeon should preserve as large an area of skin tissue as possible to cover the defect. In this case, the mass itself had a tissue expanding effect, so the flap of skin used was large enough to cover the defect. In summary, we encountered an anatomically rare presentation of schwannoma in which cosmetic considerations were important.




