

Introduction
Mesenchymal neoplasm of salivary glands are very uncommonly diagnosed and reported tumors (1.9%-4.7%) [1]. Majority of these tumors present as painless masses which grow slowly over many years [1]. Most common location of these tumors is the parotid gland (85%) and the second is the submandibular gland. On the histological view, they can be subclassified into two subgroups according to their composition : monophasic (lipoma component only) and ŌĆ£biphasicŌĆØ (lipoma component+epithelial component). Oncocytic lipoadenoma is a biphasic mesenchymal tumor, which was first described by Hirokawa et al. in 1998 [2]. It consists of adipocytes and serous acini with focal oncocytic component [3]. We herein present a case of a submandibular gland oncocytic lipoadenoma. We present the radiologic and histopathological findings of this tumor in detail to increase the understainding of this very rare tumor.
Case report
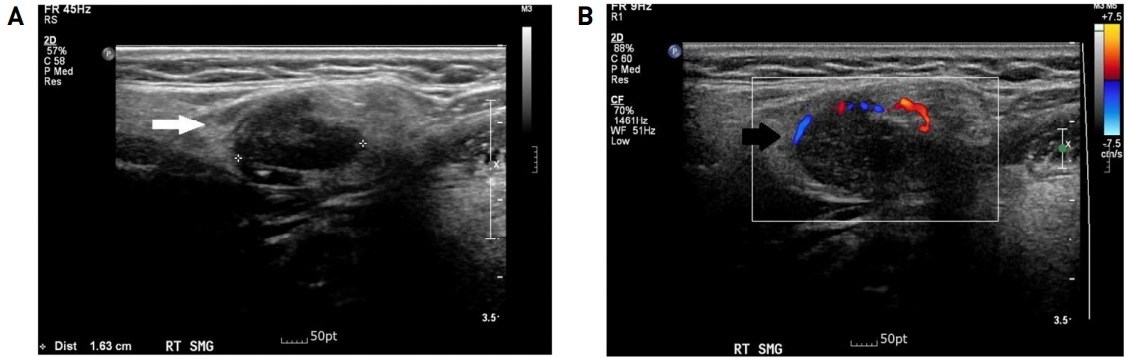
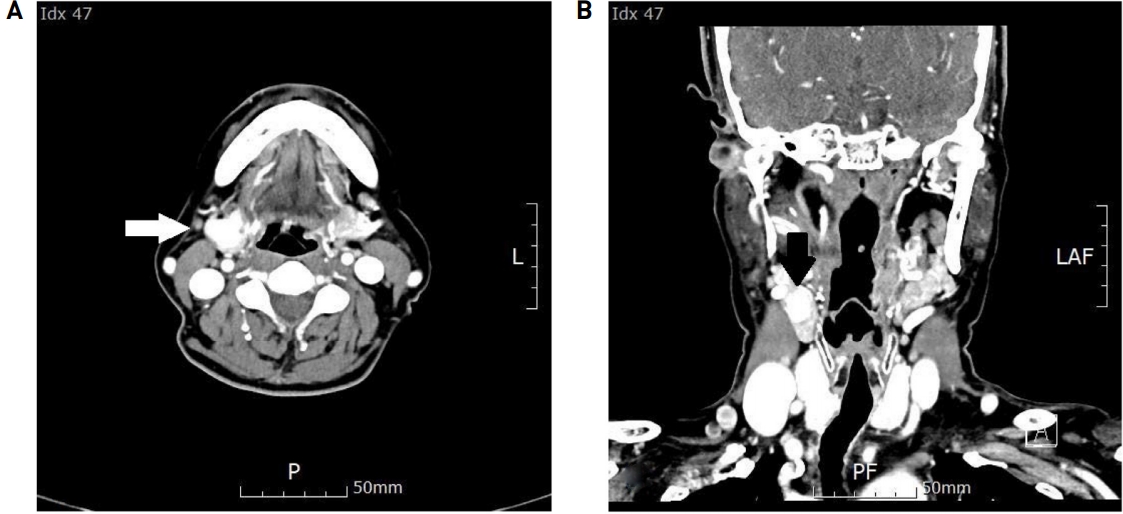
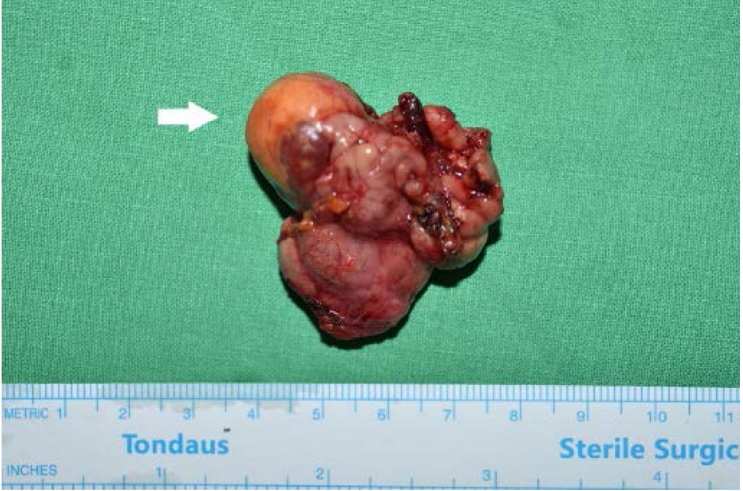
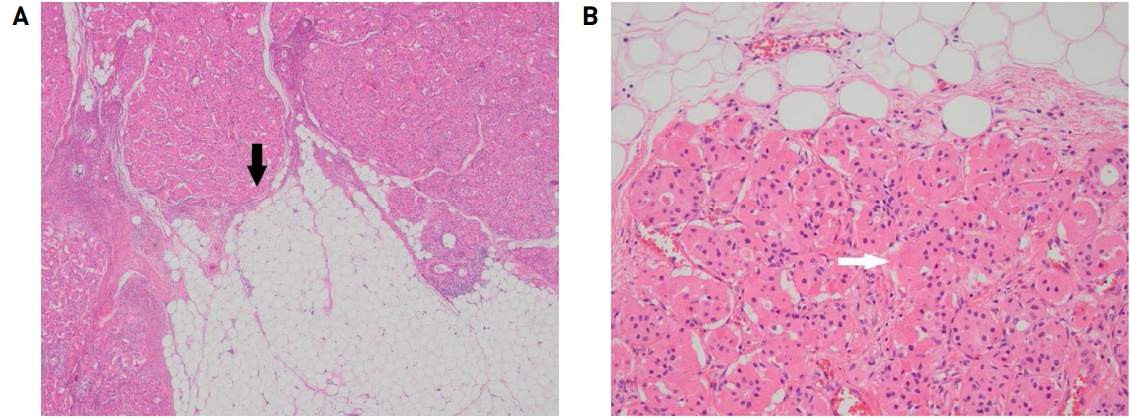
A 65-year-old female patient, without any trauma or medical history, came to the Department of Otolaryngology Head and Neck surgery with complaints of slowly growing right neck mass for four months. Physical examination revealed a 2cm sized soft and rubbery mass in right submandibular area without redness or tenderness (Fig. 1). To distinguish the swelling of right submandibular gland from tumorous condition, we performed neck ultrasound. Neck ultrasound revealed 1.6cm sized low echoic nodule in right submandibular gland (Fig. 2A) (white arrow) and color doppler image (Fig. 2B) showed the increase of vascularity along the margin of mass (black arrow). As initial impression of neck ultrasound is benign submandibular gland mass such as pleomorphic adenoma, we planned surgical excision of the submandibular gland mass. In preoperative axial CT scan (Fig. 3A) (white arrow) and coronal CT scan (Fig. 3B) (black arrow) showed about 2 x 2 x 1.6 cm sized well-defined enhancing mass containing fat component in right submandibular gland. Surgical excision was performed using usual cervical incision for submandibular gland resection without any complication. Excised surgical specimen showed about 2 (width) x 2 (thickness) x 1.6 (length) cm sized well-marginated yellowish mass abutting with submandibular gland (Fig. 4)(white arrow). The final pathologic report was oncocytic lipoadenoma. Microscopic examination revealed a well-circumscribed tumor that is surrounded by a thin, fibrous capsule. The tumor was composed of mixed population of oncocytes and adipocytes (Fig. 5A, H&E x40)(black arrow). The oncocytes were arranged in compact nests and tubules with abundant granular eosinophilic cytoplasm and small variably prominent nucleoli (Fig. 5B, H&E x 200)(white arrow). The tumor showed somewhat discrete nodules of predominant oncocytic component within lipomatous area. Cellular pleomorphism, mitoses or necrosis were not identified. Hemovac drain was removed on third day after surgical excision and the patient discharged without any complication.
Discussion
Lipomatous tumors of salivary gland can be divided into two subgroups: monophasic and biphasic subtypes. Monophasic tumors are more common, which are well circumscribed tumors with a lipomatous component only. Biphasic tumors have epithelial and a lipomatous component. Epithelial component can further be subclassified as "oncocytic" and "non-oncocytic" component. Oncocytic lipoadenoma consists of adipocytes and serous acini with focal oncocytic component [3]. The difficulty in the subclassification of these tumors may be due to the reasons that a lipomatous component may be present in pleomorphic adenoma or myoepithelioma [4]. The amount of oncocytic component may vary from tumor to tumor and even within the different areas of a tumor.
The differential diagnosis should include all the benign lipomatous salivary gland lesions. A computed tomography (CT) scan can give hints regarding the presence of a lipoma, since a density of 50-150 Hounsfield units is typical for such a tumor [5]. A magnetic resonance image may also suggest diagnosis and allows for assessment of fatty and non-fatty components [5]. Microscopic differential diagnosis of oncocytic lipoadenoma should also include lipomatosis, myoepithelioma and other salivary gland lesions with extensive lipometaplasia [6]. Lipomatosis is characterized by intensive shrinkage of acinar cells and it is a variant of interstitial lipomatosis [7]. Oncocytic lipoadenoma has a distinct enlarged main mass, which helps its separation from lipomatosis. Fibrolipoma, the second most common oral lipoma also contains mature adipose tissue [8]. Spindle cell lipoma is another lesion that needs to be distinguished from sialolipoma. It may affect the parotid region and present typically as a well-circumscribed fatty tumor with bland spindle cells, ropey collagen, and adipocytes [8]. Myoepitheliomas can consist of a single type of cells or contain a mixture of cell types lacking ductal differentiation, including spindle, plasmacytoid, epithelioid, clear, or oncocytic cell types [9]. Moreover, variable amount of myxoid, hyalinized, or clear extracellular matrix produced by myoepitheliomas, contribute to their diverse morphology [9].
The cytologic findings of oncocytic lipoadenoma described by Chahwala et al. [10] included cellular smears including oncocytic epithelial cells along with occasional fibrovascular and adipose tissue fragments in prominent lipoid background. Oncocytes may be seen in aspirates from varying conditions ranging from normal glands of elderly individuals to neoplastic lesions such as oncocytoma, oncocytic carcinoma, pleomorphic adenoma, Warthin tumor, and mucoepidermoid carcinoma [10]. For this reason, accurate diagnosis by fine-needle aspiration cytology is very difficult. Furthermore, obtaining sufficient material for accurate diagnosis is not always possible because of the bulky adipose component. Core needle biopsy can be used as a safe and effective diagnostic tool especially for lipomatous tumor in salivary gland [11].
In conclusion, we have described an uncommon case of oncocytic lipoadenoma that occurred in the submandibular gland of a 65-year-old woman. Submandibular gland lipoadenomas are extremely rare benign tumors and may be difficult to diagnose preoperatively. Physicians, surgeons, and pathologists should consider this rare disease entity especially when making a differential diagnosis of lipomatous tumor arising in salivary gland.