

Introduction
Adult fibrosarcomas are very rare and accounts for approximately 1% of adult sarcomas.1) Fibrosarcoma (FS) is a malignant tumor composed of fibroblasts with various collagens and has a herringbone structure in classical cases.2) It commonly affects the deep tissues of the limbs, trunk, head, and neck and adult FS predominantly occurs in men between 40 to 60 years of age.3) Fibrosarcomas are divided into adult-type and infantile-type fibrosarcomas according to age and prognosis.4) Some experts consider cases diagnosed before the age of two to be infantile fibrosarcomas; however, infantile fibrosarcoma usually occurs in children younger than 15 years of age.4) Since adult-type fibrosarcoma presents with aggressive features and a high rate of local tumor recurrence, accurate diagnosis and wide excision are needed for appropriate management.3) We report the follow-up and histological review of a patient who underwent wide excision and flap reconstruction for a fibrosarcoma of the left scapula region.
Case report
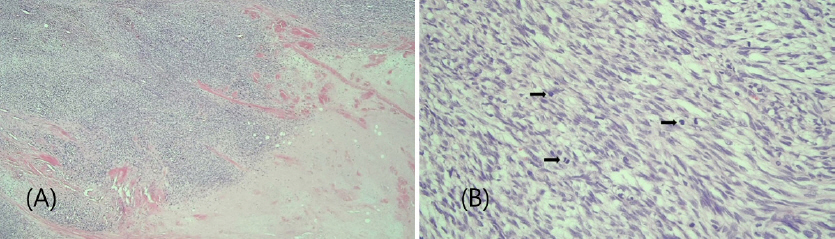
A 57-year-old man was admitted to the clinic with a palpable growing mass in the left scapular area. The examination of the patient’s back revealed a 6 cm-sized protruding pigmented tumor with a nodular surface. A soft tissue mass measuring 4.3 x 5.1 x 3.1 cm with low attenuation and mainly peripheral enhancement in the central portion was revealed by a preoperative computed tomography (CT) with contrast-enhanced imaging (Fig. 1). The punch biopsy conducted prior to the surgery showed dermal fibrosis and perivascular infiltration of lymphocytes and eosinophils. Based on the enhanced scapular CT performed prior to the surgery, there was a possibility of an epidermal inclusion cyst or soft tissue sarcoma. A wide excision surgery was planned assuming it was a dermatofibrosarcoma protuberans, which has a relatively high frequency. We performed wide excision, including the infraspinatus fascia layer with a 2 cm safety surgical margin. While the literature reports that the thickness of the central part of the infraspinatus muscle is around 5mm, this patient had been working in parcel delivery for a long period of time, resulting in relatively thicker muscle bulk. The thickness of the excised muscle was approximately 3mm. A frozen biopsy performed after wide excision revealed that the cell morphology appeared more bizarre than dermatofibrosarcoma protuberans and the base was adjacent to the malignant mass. Subsequently, a safety margin of 1.5 cm was added to dissect further below the resected area, and then, additional resection was performed in a complete bowl-shape without any opening to ensure there was no gap, considering the space that had already been resected as the form of the remaining tumor. After finding and marking the course of the circumflex scapular artery using a vascular handheld doppler, the pedicle was safely secured in the left triangular space, and a 7 × 25 cm parascapular fasciocutaneous flap was elevated and the defect was reconstructed using a parascapular propeller-type island flap (Fig. 2). Both the flap and donor site healed well without any minor complications, at the multidisciplinary consultation held on the 8th day after surgery, based on the preoperative scapular and abdominal CT scans and pathological results, no evidence of lymph node metastasis was found in the pleural cavity and other areas. Therefore, it was planned to proceed with radiation therapy first, followed by chemotherapy immediately after the completion of radiation therapy, and this plan was carried out accordingly. The resection margin was completely clear of tumor. Histopathological analysis demonstrated the spindle-shaped tumor cells with moderate degree of pleomorphism arranged in a fascicular or a “herringbone” growth pattern. The tumor shows extensive necrosis with frequent mitotic figures (34/10 high power field) and high Ki67 marker index (70%)5) (Fig. 3). Immunohistochemical staining revealed that the specimen was negative for CD34, S-100, desmin, SMA, and CD68. No evidence of distant metastatic cancer was found by positron emission tomography-CT immediately following surgery. A total of 6000cGy dose, 30 fractions of conformal radiotherapy were administered from Postoperative day (POD) 5 to 6 weeks, and a baseline study for chemotherapy conducted at POD#3months (mos) after radiation treatment was completed. Unfortunately, a CT scan revealed metastatic nodules and hematogenous lung metastasis in the left axilla, and six cycles of chemotherapy with adriamycin and ifosfamide was administered. On POD#7mos, follow-up CT revealed that the size of the metastatic lymph nodes in the left axillary region had significantly reduced, whereas multiple metastatic nodules in the right lung were observed; nine cycles of chemotherapy were further planned and implemented. A PET-CT scan performed 10 months postoperatively revealed further aggravation of the metastatic lymph node in the left axilla and metastasis in the right lung. The patient was referred to a tertiary-care hospital and underwent lymph node dissection and wedge-shaped lung resection. Consequently, axillary lymph node metastasis was confirmed again using an examination performed two years post-surgery. Upon receiving additional radiation treatment, the patient returned to the authors` institute, after a 38-month follow-up. During this period, the patient’s general condition had improved, and he returned to work before the operation. He tolerated the severe labor intensity well, and local recurrence at the surgical site was not observed. The contours of both sides of the back and the range of motion were well-maintained symmetrically (Fig. 4).
Fig. 1
Preoperative enhanced computed tomographic images. (A) Axial image and (B) sagittal image show a 4.3 x 5.1 x 3.1 cm mass, which has a central portion with low attenuation and mainly peripheral enhancement (white arrows).
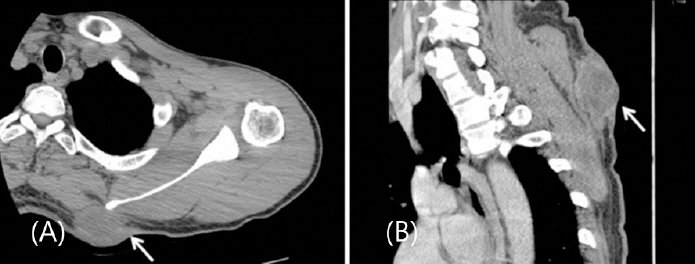
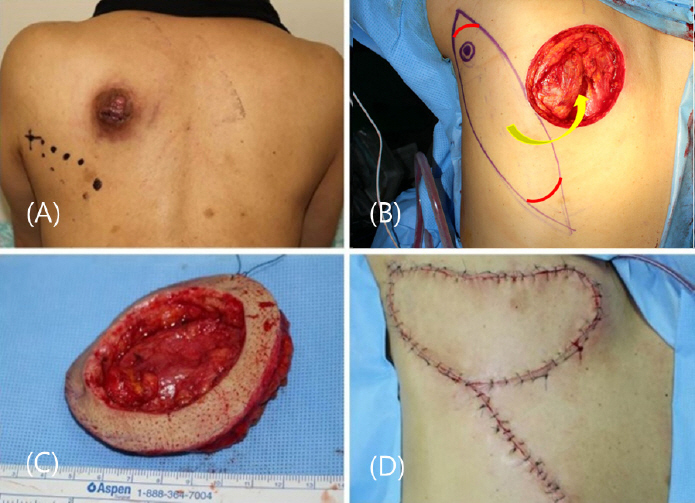
Fig. 2
Perioperative photographs. (A) Pre-operative view of a 57-year-old man, showing a 6 cm sized protruding pigmented tumor with a nodular surface on the left scapular area and a marking of the course of the circumflex scapular artery using a vascular handheld doppler. (B) Intraoperative design of the propeller-type parascapular flap. (C) Bowl-shaped additional resection. (D) Resurfacing with a parascapular island flap.

Discussion
Fibrosarcoma usually affects very deep structures and tends to originate from the intramuscular and intermuscular fibrous tissue, myofascial integument, aponeurosis, tendons, with subfascial involvement.4,6,7) Fibrosarcoma primarily occurs in areas composed of collagen-rich connective tissue; adult-type fibrosarcoma frequently develops in the lower extremities, particularly in the thighs and knees, along with the arms and trunk.6) In contrast, the diagnoses of retroperitoneal, mediastinal, and head and neck fibrosarcomas are rare.6) With the exception of dermatofibrosarcoma protuberans, fibrosarcoma arising from subcutis is rare and typically occurs in tissues damaged by radiation, heat, or scarring.7) Several tests including immunohistochemical or microstructural analysis, must be performed in addition to routine histopathological examination for an accurate diagnosis of fibrosarcoma.5) Certain mesenchymal tumors, including monophasic fibrous synovial sarcoma, leiomyosarcoma, malignant fibrous histiocytoma, malignant peripheral nerve sheath tumors, and other spindle cell tumors, have characteristics similar to those of fibrosarcoma.5) Therefore, elucidation of the typical features of this tumor subtype is crucial for accurate diagnosis.6) The exclusion of other spindle cell mesenchymal tumors is a vital step in diagnosis of fibrosarcoma in adults. Immunohistochemistry staining of adult fibrosarcoma is negative for CD34, CD99, bcl-2 and nuclear β-catenin, as well as epithelial, muscle, and neuronal markers.2) Desmin, alpha smooth muscle actin (α- SMA), and muscle-specific actin (MSA) are among the most common myogenic markers.6) Ki-67, a cell cycle-associated nuclear antigen, is also used as a prognostic marker for fibrosarcoma.6) With respect to phenotype, the cell populations were S100 and CD68 negative, excluding schwannoma and malignant fibrous histiocytoma, respectively, whereas definitely positive only for vimentin.2) Microscopic findings are important, in addition to immunohistochemistry. Adult fibrosarcoma is characterized by fusiform tumor cells with interlaced bundle formation and a herringbone pattern. Histopathological analysis in this case showed typical microscopic features of adult fibrosarcoma, with tumor cells arranged in long polycysts displaying a herringbone pattern. Immunohistochemical staining showed that the specimen was negative for CD34, S100, Desmin, SMA, and CD68, and showed a high Ki67 marker index (70%). The present case was representative of adult fibrosarcoma due to a combination of immunohistochemistry and microscopic features. The tumor did not exhibit significant skin layer changes, precluding the possibility of a fibrosarcoma area of dermal fibrosarcoma protuberans.
Radiography is crucial for defining the local extent, staging of the disease, evaluating changes after treatment, and detecting tumor recurrence. In this case, CT findings showed a homogeneous mass, weak signal amplification of the contrast media, and peripheral enhancement, suggesting fibrosarcoma.2)
A wide resection must be performed if the tumor originates from the muscle cells or grows outside the compartment.8) A margin of 2 cm is often recommended; however, a valid safety margin has generally not been established.6) Further, radiation therapy after extensive resection is highly recommended for high-grade tumors up to 5 cm in size.8) In this case, the tumor size was 5 cm with no muscle invasion. However, the base of the tumor was located adjacent to the muscle layer in the frozen biopsy obtained during the operation, and the malignancy was located higher compared to the dermatofibrosarcoma protuberance; therefore, a bowl- shaped resection was additionally performed. Consequently, a wide excision was performed, with a margin of 3.5 cm.
The defect site after tumor resection was reconstructed with a parascapular flap, which was chosen due to the absence of muscle defect in the recipient. The donor site that is adjacent to the lesion, and is a fasciocutaneous flap with reliable circulation. Barwick et al. (1982) reported that the five criteria for reconstruction of the defect using flaps: 1. applicability in a wide range of situations, 2. lengthy vascular pedicle of consistently large external diameter, 3. easy dissection, 4. minimal donor-site morbidity, and 5. uniformity of thickness and large surface dimensions.9) The parascapular flap includes the skin and can be harvested at a maximum size of 30 cm × 15 cm, with a possibility of primary suturing of the donor site. Other advantages include an intradermal network with rich anastomosis and the constant anatomy of the vessels is well-known.10) In addition, the morbidity of the donor site after surgery is low; however, a few motion limitations that are crucial for patients.11,12) During the follow-up period of three years after surgery, the patient did not experience any motional limitations, showed a symmetric back contour, and returned to daily work without functional limitations despite performing high-labor work. The patient was in very good overall condition and was working normally in delivery service. He underwent tumor removal and chemotherapy at a tertiary comprehensive hospital due to the presence of metastases in the lungs and pleura, and was under observation. Their last follow-up observation in the outpatient clinic was 3 years and 2 months ago.
To conclude, a concise histopathological diagnosis of each tumor is essential to establish a treatment plan for fibrosarcoma. This should be comprehensively determined using routine histopathological and immunohistochemical analyses. Adult-type fibrosarcoma of the scapular area is a rare case.13) The overall five-year survival rate is approximately 40-60%.6) The best prognosis should be achieved through an accurate diagnosis by the clinician, complete surgical resection of the tumor, and appropriate reconstruction. Therefore, despite a follow-up period of less than five years and metastases, there was no local recurrence, and the quality of life showed improvement. We expect that the data presented in our report may aid clinicians in handling similar challenging cases of adult FS.




